

Impact of the MAINTAIN Instrument on Clinical
Decision-making for New Spinal Pain Patients:
A Cross-sectional StudyThis section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: J Can Chiropr Assoc 2026 (Apr); 70 (1): 81–93 ~ FULL TEXT
OPEN ACCESS Patrick Boylan, DC, EdD • Andreas Eklund, DC, PhD • Leon Tom, DC • Kent Stuber, DC, PhD • Christopher A. Malaya, DC, PhD • Brandon Beckerman, DC • Per J. Palmgren, DC, PhD • Katherine A. Pohlman, DC, PhD
Logan University,
Chesterfield, MO.
The MAINTAIN instrumentObjective: This quantitative pilot study with a qualitative adjunct aimed to characterize patients at two U.S.-based chiropractic teaching clinics using the novel MAINTAIN instrument, and to assess clinicians' and interns' initial clinical impressions based on patients' MAINTAIN scores.
Methods: Between February and September 2022, 597 spinal pain patients were screened. Eligible patients (n=91) completed demographic and health questionnaires, including the MAINTAIN instrument. Clinicians and interns completed surveys to assess treatment plans and expectations for recovery. A qualitative analysis assessed clinicians' and interns' initial impressions based on patients' MAINTAIN scores.
Results: The mean MAINTAIN score was 15.06 (SD: 9.03, range -7 to 32), with 39.6% of participants identified as potential candidates for maintenance care. Qualitative analysis identified several themes and subthemes which describe how clinicians and interns used patients' MAINTAIN scores.
Conclusions: Despite limitations, these findings highlight the value of integrating the MAINTAIN instrument in chiropractic teaching clinics to enhance clinical decision-making and patient management.
Keywords: chiropractic; maintenance care; prevention; qualitative research; spinal pain.
From the FULL TEXT Article:
Introduction
Non-specific low back pain (LBP) is a highly prevalent condition with profound personal and societal consequences. It ranks among the leading causes of economic burden in Western countries. [1] LBP is frequently recurrent [2], with estimates that over two-thirds of individuals will experience a recurrence within 12 months. [3] Given its disabling nature and associated costs, implementing preventive strategies to reduce recurrence and long-term impact is both logical and necessary. [4]
Psychological [5, 6], behavioral [7], and social characteristics [8] are known to influence the progression from acute to recurrent or persistent pain states [5–12], supporting the biopsychosocial model as a foundational framework for LBP management. [8, 13–15] Chiropractors often serve as first-contact providers for both primary and recurrent spine-related pain. [16] Chiropractic maintenance care (MC) is an approach to LBP management that involves scheduled follow-up visits aimed at preventing relapse and deterioration, regardless of a patient’s symptoms. [17–28]
MC is typically initiated after the patient has achieved maximum therapeutic benefit. [17–28] Research indicates that the effectiveness of MC may be influenced by patients’ psychological, behavioral, and social profiles [29], which led to the development of the MAINTAIN instrument–a brief clinical tool designed to identify patients who may benefit from ongoing maintenance care. [4]
Educational programs in chiropractic play a crucial role in shaping clinician behavior and, consequently, patient outcomes. [30, 31] Therefore, it is important that curricula incorporate emerging evidence and tools, such as the MAINTAIN instrument, early and consistently. To our knowledge, no studies have explored how chiropractic clinicians and students use the MAINTAIN instrument to inform clinical decision-making.
The primary aim of this study was to describe the demographic and pain-related characteristics of patients presenting to chiropractic teaching clinics with recurrent or persistent spine pain, including data derived from the MAINTAIN instrument. The secondary aim was to assess clinicians’ and interns’ initial clinical impressions based on patients’ MAINTAIN scores.
Methods
Study design
This study presents cross-sectional findings from patients enrolled in a preliminary study assessing the implementation of the MAINTAIN instrument at two chiropractic teaching clinics. The methodology used a cross-sectional survey with a complementary qualitative exploration. The multi-site design involved patients, interns, and clinicians from Parker University (Dallas, TX) and Logan University (Chesterfield, MO). The study protocol was approved by the Parker University Institutional Review Board (IRB #PUIRB-2021-16) and is reported in accordance with the STROBE guidelines to ensure transparency and reproducibility of the research. [32]
Patient participation

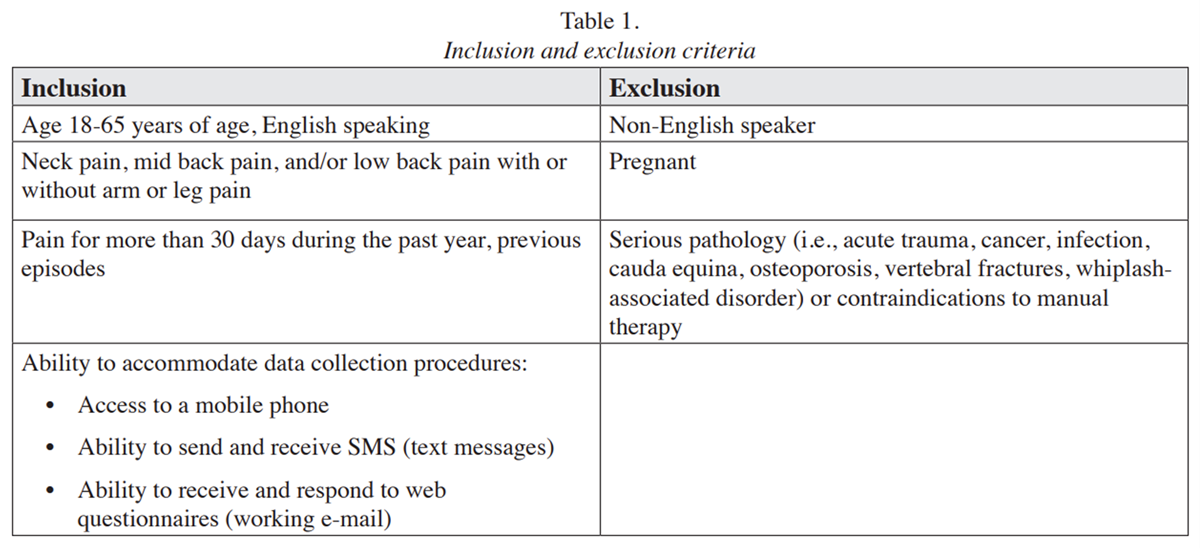
Table 1 New patients presenting with recurrent or persistent spinal pain, defined as occurring on at least 30 days in the past 12 months, were screened by participating clinicians and interns during their initial clinic visit between February and September 2022. Clinicians and interns screened patients by informing them of the study and directing them to scan a QR code on their mobile device, which was linked to the screening questionnaire. Detailed inclusion and exclusion criteria are provided in Table 1.
Patient consent and characteristics
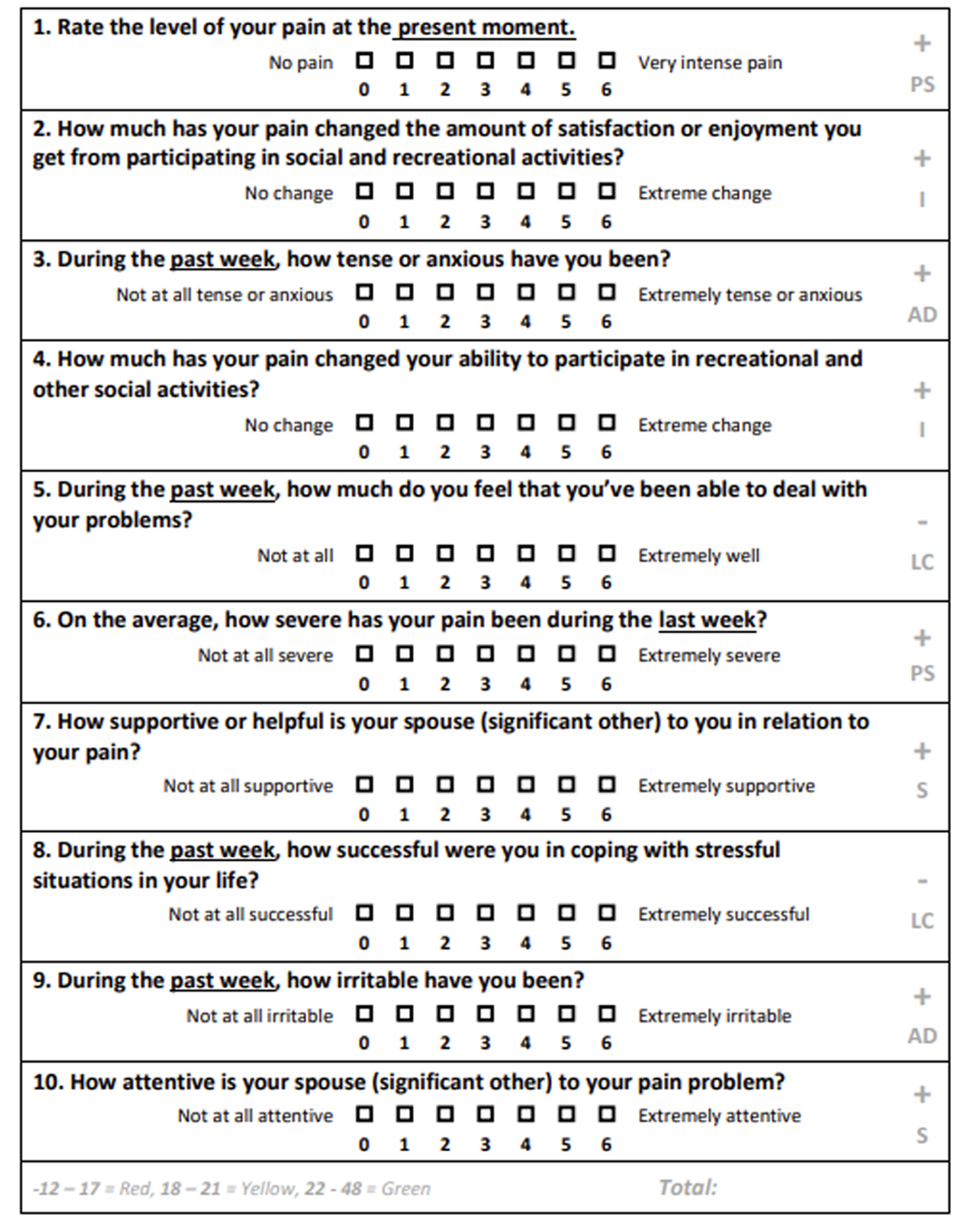
Eligible and interested patients provided informed consent and completed a baseline questionnaire prior to their initial treatment. The questionnaire included the MAINTAIN instrument and demographic and health-related outcome measures. The MAINTAIN instrument is a 10-item clinical decision aid designed to identify a patients’ likelihood of benefiting from MC with very good diagnostic accuracy. [4]Scores of 12 to 17 indicate a low likelihood of benefiting from MC;
18 to 21 indicate possible suitability, and
22 to 48 suggest a high likelihood of benefiting from MC.[4]The instrument consists of five subdomains –
pain severity,
interference,
life control,
affective distress, and
support– each item scored from 0 to 6.
Low scores are preferred for pain severity, interference, support, and affective distress subdomains, whereas higher scores are favorable for life control.
Pain intensity and disability were assessed using the Numerical Pain Rating Scale (NPRS) [33] and Roland-Morris Disability Questionnaire (RMDQ) [34], respectively.
Additional outcome measures included:
Recovery expectation, rated from 0 (no chance) to 10 (very likely)
General health, rated on a five-point scale (poor to excellent)
Pain Self-Efficacy Questionnaire (PSEQ), [36] to assess confidence in performing activities while experiencing pain, rated from 0 (not at all confident) to 6 (completely confident).
EuroQol 5D (EQ-5D-5L), [36] to assess health-related quality of life, with responses dichotomized into “no problems” or “some problems”
Clinician and intern participation
This study was conducted as part of a larger research project investigating the implementation of the MAINTAIN tool into chiropractic teaching clinics. [37] As part of the project, participating interns and clinicians were randomized into one of three groups whereby they received training on the utilization of the MAINTAIN tool in a stepwise fashion. Training consisted of either written information only in the form of an instructional handout, a one-time focused lecture on the MAINTAIN tool, or an in-depth workshop series. [37]
Clinicians and interns completed follow-up questionnaires designed to capture their clinical impressions and care planning decisions based on patient presentation and questionnaire data. The questionnaire was developed by the study authors – a multidisciplinary team of clinicians, educators, researchers, and administrators–and underwent iterative piloting and revision until consensus was achieved. Surveys were distributed via email, and respondents indicated whether the form was completed by the clinician alone, the intern alone, or collaboratively.
Each questionnaire included five closed-ended and two open-ended questions:
Closed-ended
Who is completing the survey? (clinician only/ intern only/both).
Do you think the patient is a good candidate for manual treatment? (yes/no)
Do you think the patient is a good candidate for an exercise intervention? (yes/no)
Will you treat the patient? (yes/no)
Do you expect the patient to respond to the treatment offered? (yes/no)
Open-ended
How do you plan to use the MAINTAIN score (and 5 dimensions) with this patient?
What are the treatment goals you have for this patient?
Qualitative analysis
Open-ended responses were analyzed using Braun and Clarke’s thematic analysis framework. [38] Researchers began by reviewing the responses for familiarization, followed by systematic coding of key concepts. These codes were then organized into preliminary themes, which were reviewed, refined, and defined collaboratively. The analysis process was iterative and recursive rather than strictly linear. No software was used; all coding and theme development were conducted manually. All investigators reviewed the final themes to ensure consensus. The analysis included triangulation of data and collaborative coding to ensure qualitative rigor.
Data management and analysis
All data were collected using Research Electronic Data Capture (REDCap) software. [39, 40] A convenience sampling strategy was employed, wherein participants were recruited based on their availability and willingness to participate during routine visits to the participating chiropractic teaching clinics. Descriptive statistics were calculated using STATA 14 (StataCorp. 2015. College Station, TX: StataCorp LP.). All data were stored on a secure server by one researcher (KP) to ensure confidentiality of patient information.
Results
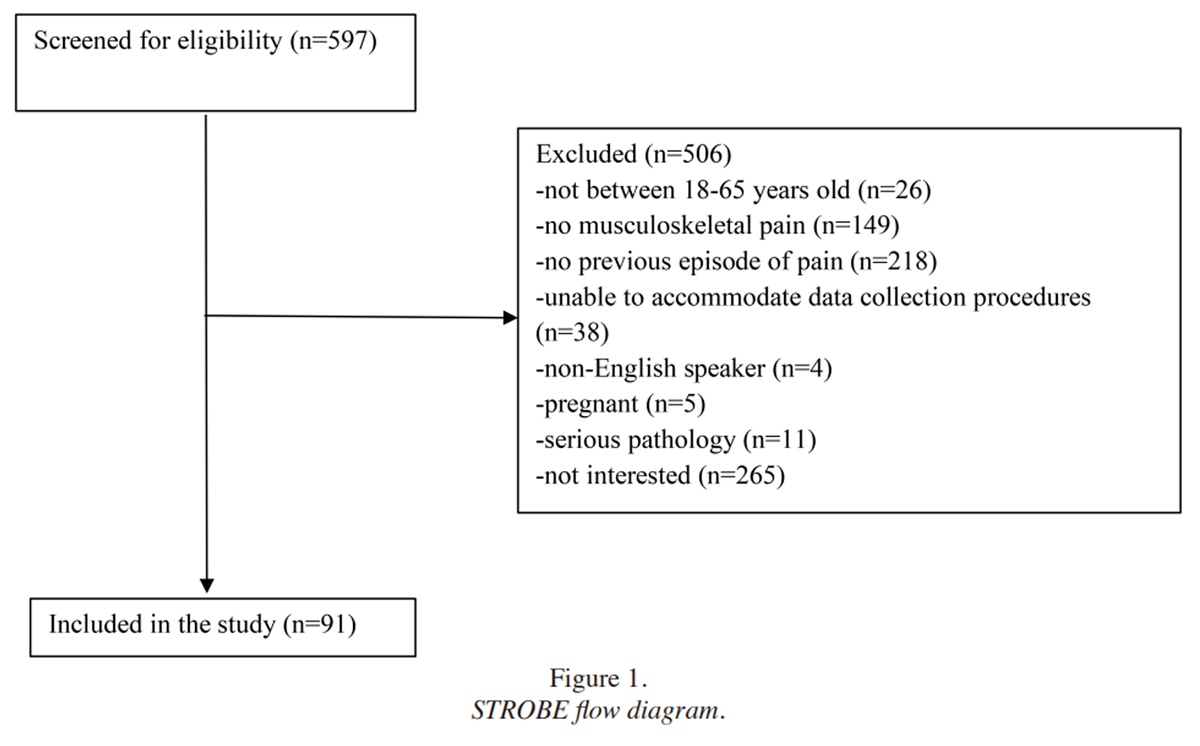
Figure 1
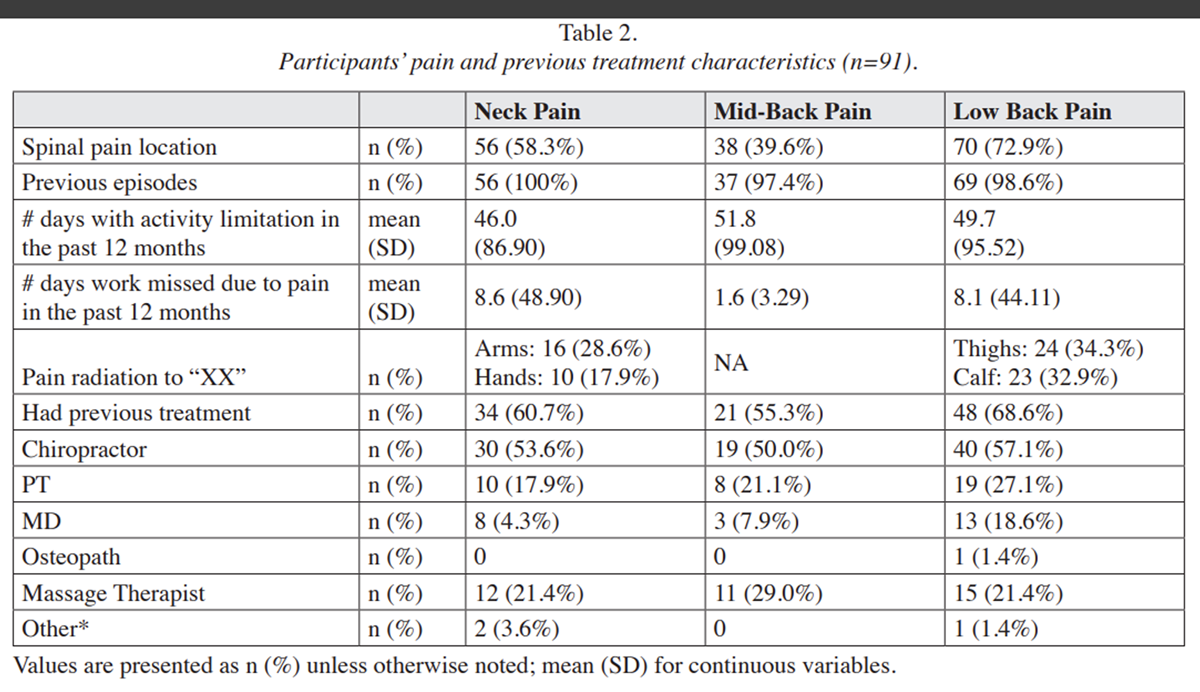
Table 2
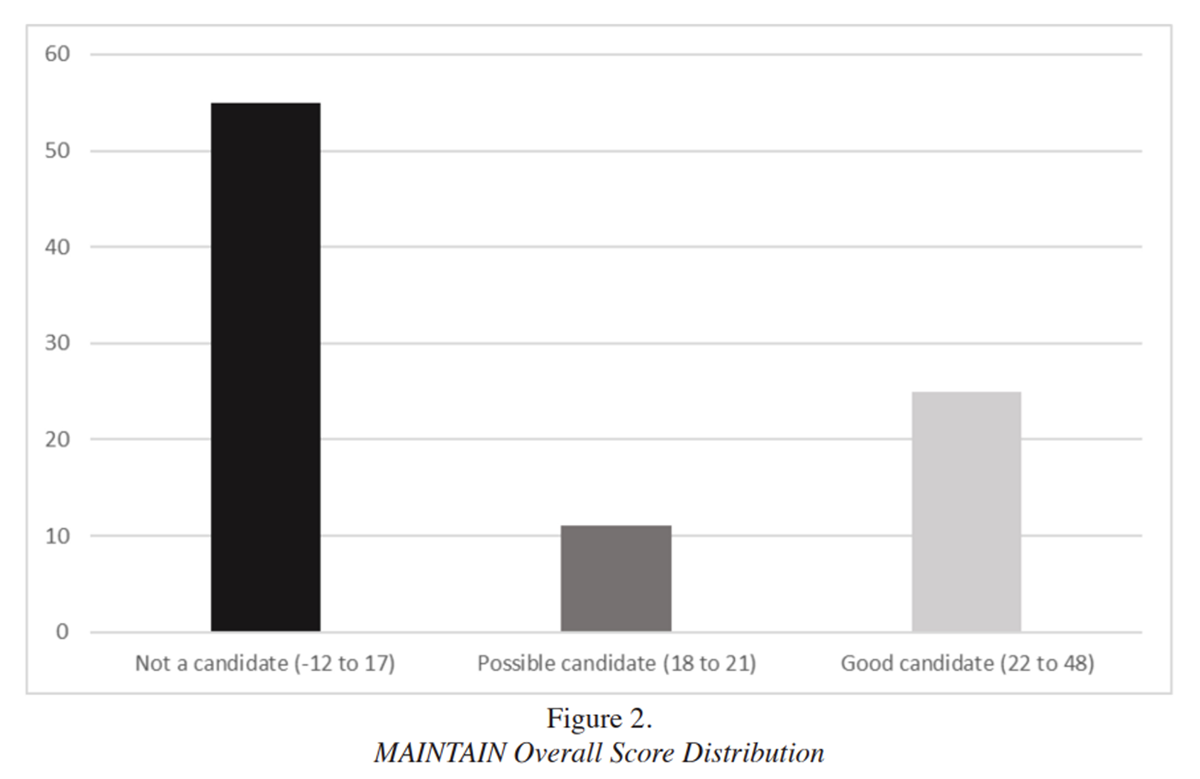
Figure 2
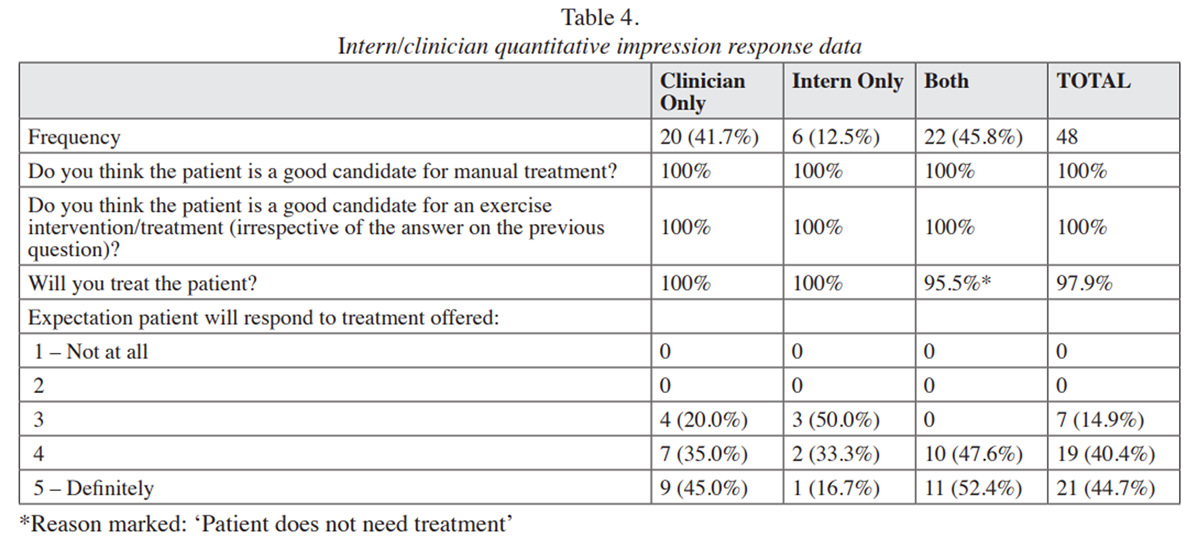
Table 3
Table 4 As shown in Figure 1, 597 patients were screened for eligibility during the enrollment period. Of those, 91 (15.2%) completed the questionnaire and were included in the analysis. Participants had a mean age of 33.7 (SD: 11.5, range: 21.1–65.7), and slightly more than half (n=51, 56.0%) were male. Pain characteristics and details of previous treatment for enrolled participants are presented in Table 2.
MAINTAIN instrument findings
Figure 2 illustrates the distribution of MAINTAIN scores among the participants. The overall mean MAINTAIN score was 15.06 (SD = 9.03), with individual scores ranging from 7 to 32. The mean (SD) subscale scores were pain severity, 5.7 (3.04); interference, 4.7 (3.01); affective distress, 5.8 (3.18); life control, 6.9 (4.80); and support, 8.1 (2.49).
Participant health characteristics
Table 3 summarizes participant health characteristics. Patients identified by the MAINTAIN instrument as possible or definite candidates for MC had comparatively poorer scores across the health-related outcome measures than those classified as not suitable candidates for MC.
Clinician and intern impressions
Table 4 summarizes the clinical impression questionnaire responses of clinicians and interns. Out of 91 baseline questionnaires distributed, 48 responses (52.7%) were received. The majority of responses were completed by the clinician only (41.7%) or by both the clinician and intern together (45.8%). All respondents deemed the patient a good candidate for manual therapy/exercise interventions. Expectations of treatment response differed between respondent groups, with expectations being lower when completed by the intern alone.
Qualitative Findings: Use of the MAINTAIN instrument
The thematic analysis of Open-ended Question 1 (How do you plan to use the MAINTAIN score (and 5 dimensions) with this patient?) revealed two overarching themes, each comprising two subthemes.The first theme, Patient Perspective, included the subthemes: Facilitating interpretation of patients’ needs and Planning for care informed by the MAINTAIN instrument.
The second theme, Treatment Management, encompassed Scaffolding communication strategies with the MAINTAIN instrument and Monitoring progress based on MAINTAIN scores. The themes and subthemes are described below with representative quotes.Patient Perspective
This theme reflects how clinicians and interns used the MAINTAIN instrument to better understand and interpret patients’ individual needs, preferences, and clinical contexts . Clinicians and interns used patient-reported experiences to guide treatment decisions, prioritize care, and plan for Maintenance Care or referrals.
Facilitating interpretation of patients’ needs
Participants frequently indicated that the MAINTAIN instrument helped identify suitable candidates for MC and provided insight into additional patient considerations. For instance, one respondent noted:“Once this patient is off of active care, we hopefully will use this questionnaire for determining proper maintenance care for her as she has other confounding issues.”
Participants also discussed using MAINTAIN subdomain scores to interpret patient needs by linking them with patient-specific clinically relevant information:
“Pain Severity: patient has severe pain after lifting heavy weights and standing more than 20 min.
Interference: Unable to workout as he would like due to pain.
Life Control: able to help pain with stretches and chiropractic treatments in the past.
Affective Distress: Anxiety in general that is medicated but not due to pain complaint.
Support: Not aware of support from significant others.”
Planning for care informed by the MAINTAIN instrument
Participants described using MAINTAIN scores to prioritize care, guide treatment planning, and consider referrals to other healthcare professionals:“Decrease pain and use affirmative language to her ADLs. Depending on patient interaction and openness, referral to mental health expert.”
Detailed treatment planning informed by MAINTAIN scores included specific interventions and visit frequencies:
“He should be a good candidate (for Maintenance Care) – we will eventually have tapering manual treatments and a home exercise program when the optimum effect of care has been achieved. They will be recommended Maintenance Care with preplanned visits at 4–12-week intervals (aiming at increasing the interval as soon as possible).”
Treatment Management
This theme captures how participants used the MAINTAIN instrument to guide communication strategies and enhance patient engagement by addressing psychosocial factors and fostering self-management. It also reflects the use of MAINTAIN scores to monitor patient progress, adjust treatment plans, and evaluate the effectiveness of care over time.
Scaffolding communication strategies with the MAINTAIN instrument
Participants used the MAINTAIN tool to determine effective communication approaches and discussion topics with patients, enhancing patient-provider interactions:“Provide patient with positive feedback and encouragement during visits to show support.”
“I plan on using this (MAINTAIN) score to measure the need for this patient to be on a wellness plan after her initial 4-week treatment or not.”Psychosocial factors identified through the MAINTAIN instrument were integrated into discussions to foster patient self-management and address underlying stressors:
“Knowing that he ranks Life Control and Support (from the MAINTAIN instrument) highly is very helpful, and I can focus my treatment plan on helping him better understand back pain and work toward self-management so that interference and distress are minimized.”
Monitoring progress based on MAINTAIN scores
Participants frequently reported intentions to use MAINTAIN scores to monitor patient progress, adjust treatments, and evaluate long-term benefit:“We will use the Maintain score to see how the patient is progressing and make changes to their treatment accordingly.”
Participants also described selectively monitoring specific MAINTAIN subdomains to evaluate progress:
“The Support category will be used to monitor the patient’s potential BPS factors that may delay or hamper the patient’s response to care.
We will utilize the Pain Severity as a baseline for which we can observe how the patient is responding to care.
Life Control will be utilized to observe how the patient is responding to care.
We will not utilize the Interference for this patient’s care.
We will not utilize affective distress for this patient’s care.”
Discussion
To our knowledge, this study represents the first prospective evaluation of the novel MAINTAIN instrument within chiropractic teaching clinics in the United States. It is also the first to explore how clinicians and interns employed the new instrument to inform clinical decision-making. In recent years, there has been a growing emphasis on integrating evidence-based practice into chiropractic curricula. [41] The MAINTAIN instrument may support this goal by providing an evidence-informed method to identify patients most likely to benefit from chiropractic MC.
We observed several demographic and clinical differences between the current patient sample and the original cohort used to develop the MAINTAIN instrument. Participants in the current study were predominantly male and generally younger than those in the Nordic Maintenance Care study conducted in Sweden. [4]
Additionally, the overall MAINTAIN scores were lower in the current study, with the majority of patients having a low likelihood of benefiting from MC. Subdomain scores also varied: participants in this study reported higher scores in pain severity, interference, support, and affective distress (subdomains where lower scores are preferred), yet also scored higher in life control (subdomains where higher scores are desirable).
These differences may be attributable to variations in demographic profiles and health characteristics between patients seen in chiropractic teaching clinic settings in the United States and typical clinical practice environments in Sweden.
Patient-centered care is characterized by care that respects and responds to individual patient preferences, needs, and values, ensuring that patient values guide all clinical decisions. [42] This approach has been increasingly recognized as vital in managing chronic and recurrent pain conditions, where treatment effectiveness often hinges on active patient engagement. [43, 44]
Shared decision-making, a collaborative process in which clinicians and patients jointly consider evidence-based treatment options alongside the patient’s preferences and circumstances, has also been identified as essential for effective chronic pain management. [45, 46]
The structured application of the MAINTAIN instrument aligns well with these patient-centered principles. Qualitative findings from this study suggest that the instrument provides individualized data that may support meaningful clinical conversations and facilitate shared decision-making. However, we did not directly observe whether this occurred during consultations.
The qualitative findings from this study also complement previous research investigating patient perceptions of MC. [47] Earlier qualitative studies involving semi-structured patient interviews identified facilitators and barriers to successful MC implementation, with patient-centered care frequently cited as a significant facilitator. Patients consistently valued care plans tailored to their circumstances and preferences, highlighting the importance of patient-centered interactions and communication strategies.
Our results similarly suggest that the systematic use of the MAINTAIN instrument supports clinicians and interns in recognizing and addressing patient-specific needs and preferences, thus enhancing the potential for successful and patient-valued MC implementation within chiropractic settings.
In addition to using MAINTAIN scores to facilitate communication and foster patient-centered clinical decision-making, our qualitative analysis shows that some participants planned to use the scores to monitor treatment effectiveness over time, which the tool has currently not been validated to do. While this could be a future direction of study in the field of MC, to date the MAINTAIN tool has not been validated for this purpose.
Clinicians and educators should exercise caution to not be overly confident in MAINTAIN scores to inform clinical decisions outside of the selection of MC candidates. A recent mixed-methods study highlights the confusion that exists regarding MC throughout chiropractic training programs [48], which could explain the misguided use of the tool observed in the current study.
Strengths and limitations
This study had several strengths. It is the first prospective evaluation of the MAINTAIN instrument in United States chiropractic teaching clinics and was conducted in a real-world clinical setting, enhancing the ecological validity of the findings. It also supports the integration of evidence-based care, aligning with current healthcare priorities. Lastly, a cross-sectional survey using quantitative and qualitative approaches was used, combining both types of data to provide richer insights.
Several limitations must be acknowledged. First, limited engagement by clinicians and interns resulted in a low screening rate, leading to low patient enrollment. Conducting research in chiropractic teaching clinics often presents unique challenges, including limited prioritization of research, inadequate institutional resources, insufficient training and faculty availability, and variable student interest. [49] Similar obstacles were encountered in the current project, which may have contributed to the limited engagement and enrollment.
Another limitation involves the generalizability of findings, as the patient health characteristics observed in chiropractic teaching clinic populations differ from those typically encountered in general clinical practice. Additionally, readers should be aware that while the MAINTAIN tool has been developed and tested on patients with low back pain, this study also included patients with neck and mid back pain, so findings should be interpreted cautiously.
Furthermore, this study employed a cross-sectional design, which restricts the ability to infer causality or evaluate changes over time. Lastly, qualitative data were obtained exclusively through written responses, which may have limited the depth of insights compared to more interactive methods such as one-to-one semi-structured interviews or focus group discussions. [50] These limitations likely impacted the study’s findings by reducing their generalizability, depth, and transferability.
Future directions
Future research should focus on improving clinician engagement through targeted training, institutional support, and practical integration of research activities into clinical routines. Including a wider variety of clinical environments, such as private practices and community-based settings, would help ensure that findings are more broadly applicable. Additionally, longitudinal study designs could offer deeper insights into how the MAINTAIN instrument influences clinical decision-making and patient outcomes over time. For qualitative research, more in-depth approaches like individual interviews or focus group discussions are recommended to capture richer, more nuanced, and transferable perspectives from both clinicians and patients.
Conclusion
This study presents the first evaluation of the MAINTAIN instrument used within chiropractic teaching clinics in the United States. It provides valuable insights into its applicability for evidence-based patient selection and tailored care planning in chiropractic MC. Despite observed demographic and clinical differences between this study’s participants and prior research populations, the results underscore the utility of the MAINTAIN instrument in promoting patient-centered care.
Specifically, the instrument facilitates the integration of psychological, social, and behavioral considerations into clinical decision-making processes The qualitative analysis further emphasizes the instrument’s role in enhancing patient-provider communication, establishing clear treatment goals, and systematically monitoring patient progress.
Although limitations related to participant engagement and uptake were encountered, this research established a foundational understanding that future investigations can build upon, exploring broader applications in clinical practice and educational contexts and informing ongoing refinement of its integration into chiropractic curricula
Conflicts of Interest:
The authors have no disclaimers, competing interests, or sources of support or funding to report in the preparation of this manuscript.
References
Hartvigsen J, Hancock MJ, Kongsted A.
What Low Back Pain Is and Why We Need to Pay Attention
Lancet. 2018 (Jun 9); 391 (10137): 2356–2367Wallwork SB, Braithwaite F, O’Keeffe M, Travers M, et al.
The clinical course of acute, subacute and persistent low back pain: a systematic review and meta-analysis.
Can Med Assoc J. 2024;196(2):E29–46.
doi: 10.1503/cmaj.230542.da Silva T, Mills K, Brown BT, Pocovi N, de Campos T, et al.
Recurrence of low back pain is common: a prospective inception cohort study.
J Physiother. 2019;65(3):159–165.
doi: 10.1016/j.jphys.2019.04.010.Eklund A, Palmgren PJ, Jakobsson U, Axén I.
Development and Evaluation of the MAINTAIN
Instrument, Selecting Patients Suitable for
Secondary or Tertiary Preventive Manual Care:
The Nordic Maintenance Care Program
Chiropractic & Manual Therapies 2022 (Mar 17); 30: 15Melzack R, Wall PD.
Pain Mechanisms: A New Theory.
Science. 1965;150(3699):971–978.
doi: 10.1126/science.150.3699.971.Hall AM, Kamper SJ, Maher CG, Latimer J, Ferreira ML, Nicholas MK.
Symptoms of depression and stress mediate the effect of pain on disability.
Pain. 2011;152(5):1044–1051.
doi: 10.1016/j.pain.2011.01.014Fordyce WE, Mosby CV.
Behavioral methods for chronic pain and illness.
Pain. 1977;3(3):291–2Sletten CD.
Psychosocial Factors in Pain: Critical Perspectives.
Mayo Clinic Proceedings. 2000;75(5):547.Hoogendoorn WE, van Poppel MNM, Bongers PM, Koes BW, Bouter LM.
Systematic Review of Psychosocial Factors at Work and Private Life as Risk Factors for Back Pain.
Spine. 2000;25(16):2114–2125.
doi: 10.1097/00007632-200008150-00017Macfarlane GJ, Thomas E, Croft PR, Papageorgiou AC.
Predictors of early improvement in low back pain amongst consulters to general practice: the influence of pre-morbid and episode-related factors.
Pain. 1999;80(1):113–119.
doi: 10.1016/s0304-3959(98)00209-7Burton AK, Tillotson KM, Main CJ, Hollis S.
Psychosocial Predictors of Outcome in Acute and Subchronic Low Back Trouble.
Spine. 1995;20(6):722–728.
doi: 10.1097/00007632-199503150-00014Linton SJ, Halldén K.
Can We Screen for Problematic Back Pain? A Screening Questionnaire for Predicting Outcome in Acute and Subacute Back Pain.
Clin J Pain. 1998;14(3):209–215.
doi: 10.1097/00002508-199809000-00007.Engel GL.
The Need For A New Medical Model:
A Challenge For Biomedicine
Science. 1977 (Apr 8); 196 (4286): 129-36Engel G.
The Clinical Application of the Biopsychosocial Model.
Am J Psych. 1980;137(5):535–544.
doi: 10.1176/ajp.137.5.535.Weiner BK.
Spine Update: the biopsychosocial model and spine care.
Spine. 2008;33(2):219–223.
doi: 10.1097/BRS.0b013e3181604572.Kosloff TM, Elton D, Shulman SA, Clarke JL, Skoufalos A.
Conservative Spine Care: Opportunities to
Improve the Quality and Value of Care
Population Health Management 2013 (Dec); 16 (6): 390–396Axén I, Rosenbaum A, Eklund A, Halasz L, Jřrgensen K, et al.
The Nordic Maintenance Care Program – Case Management
of Chiropractic Patients With Low Back Pain:
A Survey of Swedish Chiropractors
Chiropractic & Osteopathy 2008 (Jun 18); 16: 6
Review our collected Nordic Maintenance Care Program,
A Series of 17 studies published over a 15 year period.Leboeuf-Yde C, Hestbćk L.
Maintenance Care In Chiropractic –
What Do We Know?
Chiropractic & Osteopathy 2008 (May 8); 16: 3Axén I, Jensen IB, Eklund A, Halasz L, Jřrgensen K, Lange F, et al.
The Nordic Maintenance Care Program: When Do
Chiropractors Recommend Secondary and Tertiary
Preventive Care For Low Back Pain?
Chiropractic & Osteopathy 2009 (Jan 22); 17: 1Malmqvist S, Leboeuf-Yde C.
The Nordic Maintenance Care Program: Case Management
of Chiropractic Patients With Low Back Pain –
Defining the Patients Suitable for
Various Management Strategies
Chiropractic & Osteopathy 2009 (Jul 12); 17: 7Mřller LT, Hansen M, Leboeuf-Yde C.
The Nordic Maintenance Care Program – An Interview
Study on the Use of Maintenance Care in a
Selected Group of Danish Chiropractors
Chiropractic & Osteopathy 2009 (Jun 17); 17: 5Hansen SF, S Laursen AL, Jensen TS, Leboeuf-Yde C, Hestbćk L.
The Nordic Maintenance Care Program: What Are
the Indications For Maintenance Care In Patients
With Low Back Pain? A Survey of the Members
of the Danish Chiropractors' Association
Chiropractic & Osteopathy 2010 (Sep 1); 18: 25Sandnes KF, Bjřrnstad C, Leboeuf-Yde C, Hestbaek L.
The Nordic Maintenance Care Program - Time Intervals
Between Treatments of Patients With Low Back Pain:
How Close and Who Decides?
Chiropractic & Osteopathy 2010 (Mar 8); 18: 5Bringsli M, Berntzen A, Olsen D, Hestbćk L, Leboeuf-Yde C.
The Nordic Maintenance Care Program: Maintenance Care -
What Happens During the Consultation?
Observations and Patient Questionnaires
Chiropractic & Manual Therapies 2012 (Aug 10); 20 (1): 25Axén I, Bodin L.
The Nordic Maintenance Care Program: The Clinical
Use of Identified Indications for Preventive Care
Chiropractic & Manual Therapies 2013 (Mar 6); 21: 10Myburgh C, Brandborg-Olsen D, Albert H, Hestbaek L.
The Nordic Maintenance Care Program: What Is Maintenance Care?
Interview Based Survey of Danish Chiropractors
Chiropractic & Manual Therapies 2013 (Aug 20); 21: 27Eklund A, Axén I, Kongsted A, Lohela-Karlsson M, Leboeuf-Yde C, Jensen I.
Prevention of Low Back Pain: Effect, Cost-effectiveness,
and Cost-utility of Maintenance Care - Study Protocol
for a Randomized Clinical Trial
Trials. 2014 (Apr 2); 15: 102Eklund A, Jensen I, Lohela-Karlsson M, Hagberg J, Leboeuf-Yde C, et al.
The Nordic Maintenance Care Program: Effectiveness of
Chiropractic Maintenance Care Versus Symptom-guided
Treatment for Recurrent and Persistent Low Back Pain -
A Pragmatic Randomized Controlled Trial
PLoS One. 2018 (Sep 12); 13 (9): e0203029Eklund A, Jensen I, Leboeuf-Yde C, Kongsted A, Jonsson M, et al.
The Nordic Maintenance Care Program: Does Psychological
Profile Modify the Treatment Effect of a Preventive
Manual Therapy Intervention? A Secondary Analysis
of a Pragmatic Randomized Controlled Trial
PLoS One. 2019 (Oct 10); 14 (10): e0223349Childs JD, Fritz JM, Wu SS, Flynn TW, Wainner RS, Robertson EK, et al.
Implications of early and guideline adherent physical therapy for low back pain on utilization and costs.
BMC Health Serv Res. 2015;15(1)
doi: 10.1186/s12913-015-0830-3Rutten GM, Degen S, Hendriks EJ, Braspenning JC, Harting J.
Adherence to Clinical Practice Guidelines for Low Back Pain in Physical Therapy: Do Patients Benefit?
Phyl Ther. 2010;90(8):1111–1122.
doi: 10.2522/ptj.20090173vonElm E, Altman DG, Egger M, Pocock SJ, Gřtzsche PC.
Strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies.
BMJ. 2007;335(7624):806–808.
doi: 10.1136/bmj.39335.541782.ADKarcioglu O, Topacoglu H, Dikme O, Dikme O.
A Systematic Review of the Pain Scales in adults: Which to use?
Am J Emerg Med. 2018;36(4):707–714.
doi: 10.1016/j.ajem.2018.01.008Jenks A, Hoekstra T, van Tulder M, Ostelo RW.
Roland Morris Disability Questionnaire, Oswestry Disability Index, and Quebec Back Pain Disability Scale: Which has Superior Measurement Properties in Older Adults with Low Back Pain?
J Ortho Sports Phys Ther. 2022;52(7):1–29.
doi: 10.2519/jospt.2022.10802Dubé MO, Langevin P, Roy JS.
Measurement properties of the Pain Self-Efficacy Questionnaire in populations with musculoskeletal disorders: a systematic review.
PAIN Reports. 2021;6(4):e972.
doi: 10.1097/PR9.0000000000000972Feng YS, Kohlmann T, Janssen MF, Buchholz I.
Psychometric properties of the EQ-5D-5L: a systematic review of the literature.
Quality of Life Research. 2020;30(3):647–673.
doi: 10.1007/s11136-020-02688-y.Pohlman KA, Stuber KJ, Monier Z, et al.
Evaluation of chiropractic students’ perspectives on back pain management following one of three clinical evidence-based educational training interventions: a clusterrandomized trial.
J Can Chiropr Assoc. 2025;69(2):120–130Braun V, Clarke V.
Using thematic analysis in psychology.
Qualitative Res Psychol. 2006;3(2):77–101Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG.
Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support.
J Biomed Inform. 2009;42(2):377–381.
doi: 10.1016/j.jbi.2008.08.010Harris PA, Taylor R, Minor BL, Elliott V, Fernandez M, et al.
The REDCap consortium: Building an international community of software platform partners.
J Bio Inform. 2019;95(1):103208.
doi: 10.1016/j.jbi.2019.103208.Long CR, Ackerman DL, Hammerschlag R, Delagran L, et al.
Faculty Development Initiatives to Advance Research Literacy and Evidence-Based Practice at CAM Academic Institutions.
J Alt Compl Med. 2014;20(7):563–570.
doi: 10.1089/acm.2013.0385.Epstein RM, Street RL.
The Values and Value of Patient-Centered Care.
Ann Fam Med. 2011;9(2):100–103.
doi: 10.1370/afm.1239.Robinson JH, Callister LC, Berry JA, Dearing KA.
Patient-centered care and adherence: Definitions and applications to improve outcomes.
J Am Acad Nurs Pract. 2008;20(12):600–607.
doi: 10.1111/j.1745-7599.2008.00360.xO’Keeffe M, Cullinane P, Hurley J, Leahy I, Bunzli S, et al.
What Influences Patient-Therapist Interactions in Musculoskeletal Physical Therapy?
Qual Syst Rev Meta-Synthesis.
Phys Ther. 2016;96(5):609–622.
doi: 10.2522/ptj.20150240.Elwyn G.
Shared Decision Making: a Model for Clinical Practice.
J Gen Intern Med. 2012;27(10):1361–1367.
doi: 10.1007/s11606-012-2077-6.Légaré F, Adekpedjou R, Stacey D, Turcotte S, et al.
Interventions for Increasing the Use of Shared Decision Making by Healthcare Professionals.
Cochrane Database of Systematic Reviews. 2019;7(7)
doi: 10.1002/14651858.CD006732.pub4.Hjertstrand J, Palmgren PJ, Axén I, Eklund A.
The Nordic Maintenance Care Program: Patient Experience
of Maintenance Care-A Qualitative Study
Chiropractic & Manual Therapies 2021 (Aug 2); 29: 28Stuber KJ, Eklund A, Pohlman KA, Monier Z, Muller R.
Exploration of chiropractic students’ motivation toward the incorporation of new evidence on chiropractic maintenance care: a mixed methods study.
J Can Chiropr Assoc. 2024;68(2):98–112Hawk C, Cambron J, Pahmeyer D.
Issues in conducting research in chiropractic college clinics.
J Manip Physiol Ther. 2008;31(4):301–307.
doi: 10.1016/j.jmpt.2008.03.008.LaDonna KA, Taylor T, Lingard L.
Why open-ended survey questions are unlikely to support rigorous qualitative insights.
Acad Med. 2018;93(3):347–349.
doi: 10.1097/ACM.0000000000002088.
Return to MAINTENANCE CARE
Return to SPINAL PAIN MANAGEMENT
Since 6-16-2026
| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |