

Deconstructing Chronic Low Back Pain in the Older Adult -
Step by Step Evidence and Expert-Based Recommendations
for Evaluation and Treatment.
Part IX: AnxietyThis section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: Pain Med. 2016 (Aug); 17 (8): 1423–1435 ~ FULL TEXT
OPEN ACCESS Jordan F. Karp MD, Elizabeth A. DiNapoli PhD, Julie Wetherell PhD, ABPP,
Chloe Bolon BA, Eric Rodriguez MD, Joseph Shega MD, Debra K. Weiner MD
Geriatric Research, Education and Clinical Center,
VA Pittsburgh Healthcare System,
Pittsburgh, Pennsylvania Department of Psychiatry Department
of Anesthesiology Clinical and Translational Science Institute,
University of Pittsburgh,
Pittsburgh, Pennsylvania.OBJECTIVE: As a part of a series of articles designed to deconstruct chronic low back pain (CLBP) in older adults, this article focuses on anxiety-a significant contributor of reduced health-related quality of life, increased use of medical services, and heightened disability in older adults with CLBP.
METHODS: A modified Delphi technique was used to develop an algorithm for the screening and clinical care of older adults with CLBP and anxiety. A 4-member content expert panel and a nine-member primary care panel were involved in this iterative development process. Evidence underlying the recommendations is not strictly based on VA populations; therefore, the algorithm can be applied in both VHA and civilian settings. The illustrative clinical case was taken from one of the contributor's clinical practice.
RESULTS: We present a treatment algorithm and supporting tables to be used by providers treating older adults who have anxiety and CLBP. A case of an older adult with anxiety and CLBP is provided to illustrate the approach to management.
CONCLUSIONS: To promote early engagement in evidence-based treatments, providers should routinely evaluate anxiety in older adults with CLBP using a screening and treatment algorithm.
KEYWORDS: Anxiety; Avoidance Behavior; Chronic Pain; Cognitive Behavior Therapy; Fear; Low Back Pain
From the FULL TEXT Article:
Introduction
Patients with chronic low-back pain (CLBP) commonly exhibit increased levels of emotional distress. [1] For example, anxious mood and other symptoms of anxiety are commonly seen in patients with CLBP. [2] Prevalence of anxiety disorders in CLBP patients (19–31%) has been found to be greater than that of the general population (10–25%). [3–5] Polatin and colleagues (1993) also found that approximately 95% of adults with a lifetime history of anxiety disorders experienced these symptoms prior to the onset of low back pain, with only 5% reporting the development of anxiety after the onset of low–back pain. [3] Additionally, symptoms of psychological distress (e.g., anxiety and somatization) have been found to predict subsequent onset of new episodes of low back pain. [6, 7] Therefore, anxiety disorders often occur prior to and may predict the onset of CLBP. This is important from a public health perspective because co–occurring anxiety and CLBP are associated with reduced health–related quality of life, greater functional disability, increased use of medical services, and exerts a greater negative impact on patient health than either condition alone. [8–11]
According to the Diagnostic and Statistical Manual of Mental Disorders—Fifth Edition [12], anxiety disorders include syndromes that share features of excessive, persistent fear, anxiety and related behavioral disturbances that cause clinically significant distress or impairment in important areas of functioning. Depending on the type of object or situation that induces the fear or anxious response and the content of the associated thoughts or beliefs, anxiety disorders may be classified into: generalized anxiety disorder (GAD), separation anxiety, phobic avoidance, social anxiety, and panic disorder with or without agoraphobia. Anxious mood, tension, and general somatic symptoms of the sensory type have been found to be more common than other types of anxiety symptoms in CLBP patients. [2]
Anxiety and CLBP may commonly coexist due to shared neurobiology, such as common areas of brain activation [13, 14] and similar dysregulation of neurotransmitters in the central nervous system (e.g., GABA and glutamate). [15, 16] Similar psychological mechanisms may also explain the relationship between pain and anxiety, such that catastrophizing and hypervigilance may lead to amplification of physical and psychological symptoms. Indeed, high anxiety levels may heighten perception of pain and alter pain behavior in acute and chronic pain patients. [17, 18] Patients with co–existing anxiety and pain experience more severe pain and greater pain interference with activities compared to patients with pain only. [8] Kinesiophobia and pain catastrophizing (two specific forms of anxious behaviors) predict more severe pain and disability in patients with CLBP. [19]
Age can substantially influence the presentation of anxiety, including its symptomatology, prevalence, and treatment response. Late–life anxiety is frequently undiagnosed and thus untreated, particularly in patients suffering from chronic pain. This may be due to the way older adults express their anxiety which is often as general concerns about physical health, somatic symptoms, or worsening disability, and not describing physical symptoms of anxiety. [20] For example, older adults tend to worry less frequently than younger adults and have more medical and somatic complaints as opposed to psychological distress. [21, 22] Additionally, fear of falling is a common and uniquely geriatric anxiety syndrome marked by fear and avoidance of movement and physical activities. [21] Despite one in three community–dwelling older adults experiencing CLBP [23] and another 7% experiencing an anxiety syndrome [24], clinicians lack well–established guidelines for evaluation and treatment of anxiety in older adults with CLBP.
The purpose of this paper is to present an evaluation and treatment algorithm for clinicians treating older adults with co–occurring anxiety and CLBP. We also will present a case example to highlight the clinical complexities of evaluating and treating anxiety in older adults with CLBP. Since generalized anxiety disorder (GAD) is the most common anxiety syndrome in older adults [25], it is the focus of the case example.
Methods

Figure 1

Table 1
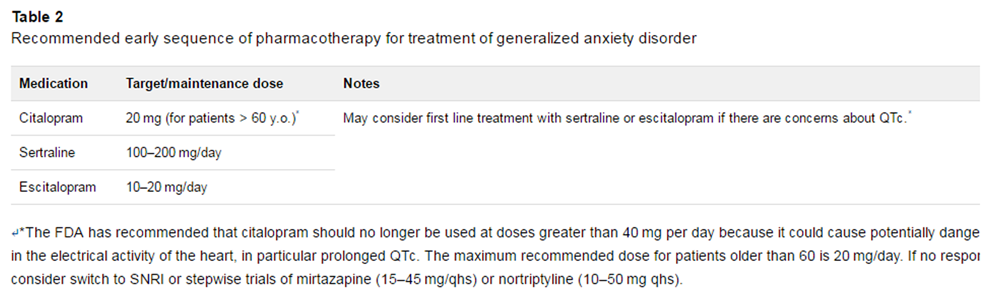
Table 2 As per the detailed description provided in the series overview [26], a modified Delphi technique involving a content expert panel and primary care review panel was used to create the CLBP and anxiety algorithm (Figure 1), the table providing the rationale for the various components of the algorithm (Table 1), and medication management recommendations (Table 2). The PI (DW) drafted an evidence–based treatment algorithm and supportive tables based upon a comprehensive review of the literature and general clinical utility when a strong evidence–based approach was not yet available. The algorithm and accompanying tables then were refined by an expert panel. Expertise represented among the 4 Delphi expert panel members included geriatric medicine, geriatric psychiatry, and geriatric psychology.
Case Presentation
Relevant Pain and Functioning History: The patient is a 76–year-old widowed black female living alone in a senior high rise who presented to her primary care physician complaining of severe low back pain. She described the pain as a constant ache (6/10 severity) that can become a sharp and stabbing pain (8/10 severity) while walking, bending, twisting, or lifting objects. Her back feels especially stiff in the morning. Her first episode of low back pain began without obvious cause 10 years ago. She has had low back pain episodically since then, however during the past 2 years the low back pain has worsened and is present more days than not. She is unable to walk more than two blocks at a time or stand for more than several minutes without severe pain. The low back pain limits her ability to function independently and her two daughters have been assisting her with transportation, groceries, and accompanying her to doctor appointments. When asked how she spends her day, she replied, “I used to be more active, now I am alone puttering at home more often than not.” The patient described being fearful of walking up the stairs to her bedroom because of fear of falling because “the pain might overwhelm me, making me feel weak,” and she is concerned that excessive activity will damage her spine.
She has consulted both a neurological surgeon and orthopedic surgeon during the past 5 years to inquire if surgery may help with her low back pain. While equivocal, both surgeons suggested she consider laminectomy and fusion. Because of anxiety about being able to manage on her own after surgery and worries that the surgery might not work, she has never had spine surgery. Over the past 4 years she episodically consulted pain medicine specialists at a pain clinic where she was treated with opioid analgesics, non-opioid analgesics, and muscle relaxants. She tried physical therapy 2 years ago, but felt it exacerbated the pain. She has used heat therapy, massage therapy, and topical analgesics. Currently she is prescribed cyclobenzaprine 10 mg TID, gabapentin 900 mg TID, oxycontin 10 mg BID, and alprazolam 0.5 mg up to TID as needed.
Relevant Physical and Psychiatric Examination, and Review of Symptoms: She was alert and oriented X 5. Her thought process was tangential but redirectable. She carried a quad cane in her left hand, and her stride length was short with a slow gait. Examination of paralumbar erector spinae musculature was notable for exquisite tenderness with taut bands and trigger points bilaterally that when palpated reproduced the patient’s pain. She appeared frail and her body mass index was 20. Her Mini Mental State Examination score was 29 (theoretical range is 0–30), missing 1-point for not knowing the county. [27] She scored a 15 on the Generalized Anxiety Disorder 7-item scale (theoretical range 0–21) endorsing daily anxiety, worrying too much about different things, being unable to stop worrying, and feeling afraid as if something awful might happen. [28] More than half the days she has trouble relaxing. She spontaneously reported that she has always been a poor sleeper, but is now having increasing difficulty falling asleep despite taking the 0.5 mg of alprazolam before bed every night as she has for many years. She said that she worries most at night while she is trying to fall asleep. She described using alprazolam and prayer to help manage excessive worry. The Patient Health Questionnaire (PHQ-9) was administered to assess for depression. [29] She scored a 9 (theoretical range 0–27), which is indicative of mild depressive symptoms. She endorsed the following: insomnia and poor appetite more than half the days, and mild symptoms of low energy, poor concentration, self-critical thinking, and restlessness. She did not meet criteria for a depressive disorder, denying depressed mood, anhedonia, or suicidal ideation, saying, “I love being alive, I’m just so worried that something bad is going to happen, or I will fall.” She denied stockpiling pills or misusing her medications. She completely abstains from alcohol. Upon further discussion, she reported that she is increasingly worried about her health and what will happen “when my pain gets too bad that I can’t walk—my daughters will have to push me in a wheelchair.” In addition to her CLBP, she described concerns about bowel functioning, frequent nausea, headaches, fatigue, and tingling in her hands and feet. She denied fever, chills, night sweats, or weight change. The main identified contributors to the patient’s CLBP were Generalized Anxiety Disorder (GAD) and myofascial pain syndrome.
Approach to Management
Many older adults with clinically significant anxiety have not been previously diagnosed with an anxiety disorder and may not spontaneously report symptoms of anxiety. [30] Given the high comorbidity of anxiety and low back pain and the potential benefits of treatment, we recommend screening for anxiety with the GAD-2 [28] in all older adults with CLBP. Brief screeners (2-items), such as the GAD-2, have been found to be equally sensitive and specific at detecting anxiety in CLBP patients compared to widely used longer-form “gold standards”. [28, 31-33] If patients score a 3 or greater on the GAD-2, providers should conduct a more thorough assessment of anxiety severity by using the GAD-7 [28], which provides more granular details about anxiety that is not routinely ascertained during medical visits. Using the threshold score of 10, the GAD-7 has a sensitivity of 89% and a specificity of 82% for GAD. [34] For patients that were positive on the brief screener (i.e., GAD-2 ≥ 3) but more thorough assessment was negative for anxiety (i.e., GAD-7 < 10), it is recommended that providers administer annual GAD-2 screenings to these at-risk patients as an efficient way to identify syndromal anxiety in patients who may not spontaneously report it. The patient presented above spontaneously reported anxiety symptoms, thus the GAD-7 was performed without first doing the GAD-2. Somatic complaints accompanying anxiety often support a diagnosis of GAD rather than other anxiety disorders. When excessive somatic complaints are present, patients may also meet criteria for Illness Anxiety Disorder. [12] It is not uncommon for anxious older adults to have more than one anxiety disorder, which may be treated simultaneously.
Another approach for providers to screen for anxiety in older adults with CLBP is to assess whether the patient is taking benzodiazepines, sedatives, and/or over-the-counter sleep aids on a regular basis. Long-term benzodiazepine and sedative use is common, particularly in primary care settings, yet considered to be relatively unsafe for older adults. [35, 36] Even low doses of benzodiazepines in older adults may lead to negative outcomes, such as increased risk of falls, fractures, cognitive impairment, and delirium. [37] If benzodiazepines or sedatives are prescribed, we recommend providers refer to the Beers criteria for appropriateness of prescribing as well as consider working with a specialist to reduce benzodiazepine use in cases of dependence. Discontinuing benzodiazepines that have been prescribed long-term is often challenging because of physiological withdrawal, psychological dependence, and need to monitor for the return and clinical management of anxiety symptoms. [38, 39]
When treatment is warranted (i.e., current diagnosis of anxiety or GAD-7 ≥ 10), both selective serotonin reuptake inhibitors (SSRIs) and cognitive behavioral therapy (CBT) are effective for treating anxiety in older adults. [40-42] Using a shared-decision making approach (i.e., a collaborative process where patients and their providers make health care decisions together), providers may implement treatment with a SSRI (Table 2), CBT, or both. While SSRIs are superior to placebo [43, 44], the benefits of pharmacotherapy may not be as durable as the skills acquired with psychotherapy. CBT may not only boost treatment response for partial responders to an SSRI but may also allow for patients to discontinue their SSRI while maintaining adequate symptom control. [21] When pharmacotherapy is the preferred treatment method, it is recommended that SSRIs be used first-line. If patients do not respond, providers may then consider switching to a serotonin-norepinephrine reuptake inhibitor (SNRI) or another agent such as mirtazapine or nortriptyline (i.e., consider stepwise trial of mirtazapine (15–45 mg/qhs) or nortriptyline (10–50 mg qhs)). When treatment is initiated, whether it is pharmacotherapy or psychotherapy, providers should utilize a measurement-guided approach, monitoring for clinically meaningful response with the GAD-7 (scores of ? 5) or the Penn State Worry Questionnaire-abbreviated version (improvements of 6 points). [45] If anxiety is disabling and/or does not respond to these interventions, providers should consider a referral to Behavioral Health or Psychiatry. On an annual basis, providers should assess benefits of sustained exposure to medication versus risk of relapse if discontinued.
Older adults with an anxiety disorder are frequently diagnosed with a comorbid depressive or insomnia disorder [46, 47] and if present, such disorders should be treated concurrently as described in the Depression and Insomnia articles in this series. [48, 49] In addition, some older adults may misuse opioids in an effort to alleviate anxiety. Given the risks of prolonged exposure to opioids in older adults (e.g., falls, sedation, respiratory depression), and that opioids are not an approved treatment for anxiety, a taper of opioids may be indicated.
Resolution of Case
The patient’s primary care physician reviewed the common symptoms of GAD with her and her daughter. The patient was resistant to the idea that anxiety may worsen her experience of pain, but her daughter reinforced that she has observed this pattern—that when her mother is more anxious, often in response to family stress and concerns about money, she often experiences a pain flare and becomes less physically active. The provider also explained to the patient that her current medications—cyclobenzaprine, alprazolam, and oxycontin—may increase her risk of falls and cognitive impairment and pointed out that these medications do not seem to be providing adequate analgesia. The patient stated “Yes, but they take the edge off. Without them I would be in even worse shape.”
After describing the various treatment options for anxiety, the patient and provider mutually decided that to treat her symptoms of anxiety she would be prescribed escitalopram 10 mg/day. At first, the patient was apprehensive about taking an antidepressant, claiming “I’m not depressed.” She was fearful about side effects (e.g., weight gain and interactions with other medication) and if the medication would be addictive. Her provider explained to her that antidepressants are approved for the treatment of anxiety in addition to depression. The daughter agreed to provide ongoing encouragement to her mother to take the escitalopram every day. The patient was offered a referral to a psychologist for CBT, but she refused. She did agree, however, to join a gentle yoga and meditation group at their church, and the daughter agreed to attend with her on a weekly basis. Relaxation approaches, such as yoga and meditation, have been found to be the most effective component of CBT for anxiety in older adults. [50]
At the first follow-up visit 2 weeks later, the patient reported experiencing nausea, “palpitations,” and “wooziness” after taking the first dose of escitalopram 10 mg and stopped taking it after that first dose. She agreed to a much slower titration, starting at 2.5 mg for the first week, increasing by 2.5 mg every 7 days. She tolerated this slow titration quite well, and after taking the 10 mg dose for 6 weeks, stated that she felt that her “mind is not racing all the time—I’m settled now.” She continued to endorse daily low back pain, but denied any recent flares and was less fearful about movement and the future. She attended the gentle yoga/meditation group with her daughter and was following recommendations of the instructor to use deep breathing and progressive muscle relaxation techniques for at least 15 minutes every day. After 2 months of treatment, the provider assessed the patient’s progress with treatment with the GAD-7 and she scored a 5, which indicated an improvement from her initial assessment. She described feeling “peaceful” after practicing the deep breathing and progressive muscle relaxation exercises, and was committed to continuing this practice. While she refused to stop taking the alprazolam for sleep, she did agree to decrease daytime use. Although the patient was fearful of stopping use of opioids over the course of four months, the long acting oxycontin was gradually discontinued. Since there is insufficient evidence to support the efficacy of cyclobenzaprine for myofascial syndromes [51], and cyclobenzaprine is listed on the Beers list as a medication to avoid in older adults, this medication was also discontinued over the course of four months. This slow taper of these medications did not result in worsening of her pain. Despite limited evidence that gabapentin improves myofascial pain, and acknowledging that it is not approved for treatment of anxiety [52], since the patient did not want to discontinue the gabapentin and was tolerating it well, because of perceived benefit, her physician agreed to continue its use.
It also should be highlighted that this patient had both anxiety and myofascial pain (MP) as important contributors to her CLBP. Anxiety is thought to be an important perpetuating factor in patients with MP. [53] Anxiety symptoms are common in patient with MP [54], and our own preliminary data (not shown) suggest that one in two older veterans with MP as part of their CLBP also has significant anxiety symptoms. Anxiety may cause muscle tension [55] that contributes to MP, and it can contribute to central sensitization, thought to be an important contributor to MP pathogenesis. [56] The pharmacological and behavioral treatment of our patient’s anxiety likely contributed to improving her MP and the lessening frequency of her pain flares.
Summary
Symptoms of anxiety are common in older adults with CLBP and the co-occurrence of these disorders is associated with negative patient outcomes such as amplified disability and overuse of opioids and benzodiazepines. Unfortunately, late-life anxiety is often undiagnosed and thus undertreated, particularly in chronic pain patients. Therefore, it is paramount that providers routinely screen for anxiety in older adults with CLBP to identify patients who may benefit from treatment (i.e., SSRIs or CBT). Recently, the US task force released recommendations for screening of depression in adults. [57] Even though this statement did not include assessing for other commonly occurring symptoms of emotional distress, such as anxiety, we believe joint screening (i.e., anxiety and depression) may be efficiently done with this high-risk group of older adults. The goal of the treatment algorithm (Figure 1) is to provide an evidence-based decision aid for clinicians to use in the shared treatment decision-making process with older adults with co-occurring anxiety and CLBP.
Older adults with CLBP commonly exhibit increased levels of emotional and cognitive distress. In addition, patients with anxiety and CLBP are at increased risk for having co-occurring mental health conditions, such as depression, insomnia and substance use. Given the complexity of such patients, it is important that providers assess and treat these mental health conditions while concurrently treating anxiety. Because they are associated with negative patient outcomes, providers also need to assess for whether the patient is taking long-term benzodiazepines, sedatives, and/or over-the-counter sleep aids on a regular basis. If such medications are prescribed in older adults with co-occurring anxiety and CLBP, it is recommended that providers refer to the Beers criteria for appropriateness and consider discontinuing their use, possibly with guidance from Behavioral Health specialists.
Key Points
Co-occurring anxiety and CLBP have been linked with negative outcomes such as greater functional disability, reduced health-related quality of life, overuse of benzodiazepines, and misuse of opioids. Therefore, clinical evaluation of all older adults with CLBP should include screening for anxiety.
Treatment algorithms to guide management of anxiety in patients with CLBP may increase recognition of patients in need of treatment as well as increase their engagement in evidence-based treatments.
Long-term use of benzodiazepines, sedatives, and OTC sleep aids for treatment of anxiety or pain should be avoided in older adults. They also may be indicative of an underlying anxiety disorder.
Treatment recommendations should be guided by collaboration with the patient to determine shared treatment goals and preferences. First-line treatment options include pharmacotherapy with SSRIs or psychotherapy using a cognitive behavioral approach.
Anxiety can contribute to muscle tension and myofascial pain. Thus, anxiety is an important treatment target in patients with a myofascial contributor to CLBP.
Funding sources:
This material is based on work supported by the Department of Veterans Affairs, Veterans Health Administration, Office of Research and Development, Rehabilitation Research and Development Service.
Disclosure and conflicts of interest:
The contents of this report do not represent the views of the Department of Veterans Affairs or the United States government. There are no conflicts of interest to report.
References:
Waddell G, Main CJ, Morris EW, Paola M, Gray I. Chronic low-back pain, psychological distress, and illness behavior. Spine 1984;9(2):209–13
Krishnan KRR, France RD, Pelton S, et al. Chronic pain and depression. II. Symptoms of anxiety in chronic low back pain patients and their relationship to subtypes of depression. Pain 1985;22:289–94
Polatin PB, Kinney RK, Gatchel RJ, Lillo E, Mayer TG. Psychiatric illness and chronic low-back pain: The mind and the spine—Which goes first? Spine 1993;18(1):66–71
Robins L, Helzer J, Weissman M, et al. Lifetime prevalence of specific psychiatric disorders in three sites. Arch Gen Psychiatry 1984;41:949–58
Atkinson JH, Slater MA, Patterson TL, Grant I, Garfin SR. Prevalence, onset, and risk of psychiatric disorders in men with chronic low back pain: A controlled study. Pain 1991;45:111–21
Croft PR, Papageorgiou AC, Ferry S, et al. Psychological distress and low back pain: Evidence from a prospective study in the general population. Spine 1996;20(24):2731–7
Pincus T, Burton K, Vogel S, Field AP. A systematic review of psychological factors as predictors of chronicity/disability in prospective cohorts of low back pain. Spine 2002;27(5):E109–20
Bair MJ, Wu J, Damush TM, Sutherland JM, Kroenke K. Association of depression and anxiety alone and in the combination with chronic musculoskeletal pain in primary care patients. Psychosom Med 2008;70(8):890–7
Kroenke K, Outcalt S, Krebs E, et al. Association between anxiety, health-related quality of life and functional impairment in primary care patients with chronic pain. Gen Hosp Psychiatry 2013;35:359–65
Levinson D, Karger CJ, Haklai Z. Chronic physical conditions and use of health services among persons with mental disorders: Results from the Israel national health survey. Gen Hosp Psychiatry 2008;30(3):226–32
Salazar A, Duenas M, Antonio J, et al. Undiagnosed mood disorders and sleep disturbances in primary care patients with chronic musculoskeletal pain. Pain Med 2013;14:1416–25
American Psychiatric Association. DSM 5. Washington, DC: American Psychiatric Association, 2013.
Porro CA. Functional imaging and pain: Behavior, perception, and modulation. Neuroscientist 2003;9:354–69
Grachev ID, Fredrickson BE, Apkarian AV. Brain chemistry reflects dual states of pain and anxiety in chronic low back pain. J Neural Transm 2002;109:1309–34
Bras M, Dordevic V, Gregurek R, Bulajic M. Neurobiological and clinical relationship between psychiatric disorders and chronic pain. Psychiatria Danub 2010;22(2):221–6
Von Korff M, Dworkin SF, Le RL, Kruger A. An epidemiologic comparison of pain complaints. Pain 1988;32:173–83
Kain ZN, Sevarino F, Alexander GM, Pincus S, Mayes LC. Preoperative anxiety and postoperative pain in women undergoing hysterectomy: A repeated-measures design. J Psychosom Res 2000;49(6):417–22
van den Hout JH, Vlaeyen JW, Houben R, Soeters AP, Peters ML. The effects of failure feedback and pain-related fear on pain report, pain tolerance, and pain avoidance in chronic low back pain patients. Pain 2001;92(1):247–57
Picavet HS, Vlaeyen JW, Schouten JS. Pain catastrophizing and kinesiophobia: Predictors of chronic low back pain. Am J Epidemiol 2002;156:1028–34
Miloyan B, Byrne GJ, Pachana NA. Age-related changes in generalized anxiety disorder symptoms. Int Psychogeriatr 2014;26:565–72
Wetherell JL, Petkus AJ, White KS, et al. Antidepressant medication augmented with cognitive behavioral therapy for generalized anxiety disorder in older adults. Am J Psychiatry 2013;170:782–9
Goncalves DC, Byrne GJ. Who worries most? Worry prevalence and patterns across the lifespan. Int J Geriatr Psychiatry 2013;28:41–9
Weiner DK, Haggerty CL, Kritchevsky SB, et al. How does low back pain impact physical function in independent, well-functioning older adults? Evidence from the health ABC cohort and implications for the future. Pain Med 2003;4(4):311–20
Gum AM, King-Kallimanis B, Kohn R. Prevalence of mood, anxiety, substance-abuse disorders for Americans in the national comorbidity survey-replication. Am J Geriatr Psychiatry 2009;17:782–92
Byers AL, Yaffe K, Covinsky KE, Friedman MB, Bruce ML. High occurrence of mood and anxiety disorders among older adults: The National Comorbidity Survey Replication. Arch Gen Psychiatry 2010;67:489–96
Weiner DK.
Deconstructing Chronic Low Back Pain in the Older Adult -
Shifting the Paradigm from the Spine to the Person
Pain Med 2015; 16 (5): 881–885Folstein MF, Folstein SE, McHugh PR. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res 1975;12(3):189–98
Spitzer RL, Kroenke K, Williams JBW. Lowe B. A brief measure for assessing generalized anxiety disorder. Arch Intern Med 2006;166:1092–7
Kroenke K, Spitzer R, Williams W. The PHQ-9: Validity of a brief depression severity measure. J Gen Int Med 2001;1:606–16
Wolitzky-Taylor KB, Castriotta N, Lenze EJ, Stanley MA, Craske MG. Anxiety disorders in older adults: A comprehensive review. Depress Anxiety 2010;27(2):190–211
Reme SE, Lie SA, Eriksen HR. Are 2 questions enough to screen for depression and anxiety in patients with chronic low back pain? Spine 2014;39(7):455–62
Mohlman J, Bryant C, Lenze EJ, et al. Improving recognition of late life anxiety disorders in diagnositc and statistical manual of mental disorders, fifth edition: Observations and recommendations of the advisory committee to the lifespan disorders work group. Int J Geriatr Psychiatry 2012;27(6):549–56
Wild B, Eckl A, Herzog W, et al. Assessing generalized anxiety disorder in elderly people using the GAD-7 and GAD-2 scales: Results of a validation study. Am J Geriatr Psychiatry 2013;22(10):1029–38
Kroenke K, Spitzer RL, Williams JBW, Monahan PO, Löwe B. Anxiety disorders in primary care: Prevalence, impairment, comorbidity, and detection. Ann Intern Med 2007;146(5):317–25
Airaksinen O, Brox JI, Cedraschi C, Hildebrandt J, Klaber-Moffett J, Kovacs F, et al.
Chapter 4. European Guidelines for the Management of Chronic Nonspecific Low Back Pain
European Spine Journal 2006 (Mar); 15 Suppl 2: S192–S300Campanelli CM. American geriatrics society updated beers criteria for potentially inappropriate medication use in older adults: The American geriatrics society 2012 beers criteria update expert panel. J Am Geriatr Soc 2012;60(4):616–31
Simon GE, Ludman EJ. Outcome of new benzodiazepine prescriptions to older adults in primary care. Gen Hosp Psychiatry 2006;28(5):374–8
Parr JM, Kavanagh DJ, Cahill L, Mitchell G, McD Young R. Effectiveness of current treatment approaches for benzodiazepine discontinuation: A meta-analysis. Addiction 2009;104(1):13–24
Baillargeon L, Landreville P, Verreault R, et al. Discontinuation of benzodiazepines among older insomniac adults treated with cognitive-behavioural therapy combined with gradual tapering: A randomized trail. CMAJ 2003;169:1015–20
Lenze EJ, Rollman BL, Shear MK, et al. Escitalopram for older adults with generalized anxiety disorder: A randomized controlled trial. JAMA 2009;301(3):295–303
Goncalves DC, Bryne GJ. Interventions for generalized anxiety disorder in older adults: Systematic review and meta-analysis. J Anxiety Disord 2012;26(1):1–11
Gould RL, Coulson MC, Howard RJ. Efficacy of cognitive behavioral therapy for anxiety disorders in older people: A meta-analysis and meta-regression of randomized controlled trials. J Am Geriatr Soc 2012;60(2):218–29
Lenze EJ, Mulsant BH, Shear MK, et al. Efficacy and tolerability of citalopram in the treatment of late-life anxiety disorders: Results from an 8-week randomized, placebo-controlled trial. Am J Psychiatry 2004;162(1):146–50
Schuurmans J, Comijs H, Emmelkamp PM, et al. A randomized controlled trial of the effectiveness of cognitive-behavioral therapy and sertraline versus waitlist control group for anxiety disorders in older adults. Am J Geriatr Psychiatry 2006;14(3):255–63
Hopko DR, Reas DL, Beck J, et al. Assessing worry in older adults: Confirmatory factor analysis of the penn state worry questionnaire and psychometric properties of an abbreviated model. Psychol Assess 2003;15(2):173–83
Schoevers RA, Deeg DJH, van Tilburg W, Beekman ATF. Depression and generalized anxiety disorder: Co-occurrence and longitudinal patterns in elderly patients. Am J Geriatr Psychiatry 2005;13:31–9
Brenes GA, Miller MM, Stanley MA, et al. Insomnia in older adults with generalized anxiety disorder. Am J Geriatr Psychiatry 2009;17(6):465–72
Carley J, Karp JF, Gentili A, et al.
Deconstructing Chronic Low Back Pain in the Older Adult - Step by Step
Evidence and Expert-Based Recommendations for Evaluation and Treatment.
Part IV: Depression
Pain Medicine 2015 (Nov); 16 (11): 2098–2108Bramoweth AD, Renqvist JG, Germain A, et al.
Deconstructing Chronic Low Back Pain in the Older Adult - Step by Step
Evidence and Expert-Based Recommendations for Evaluation and Treatment.
Part VII: Insomnia
Pain Medicine 2016 (May); 17 (5): 851–863Thorp SR, Ayers CR, Nuevo R, et al. Meta-analysis comparing different behavioral treatments for late-life anxiety. Am J Geriatr Psychiatry 2009;17(2):105–15
Leite FM, Atallah AN, El Dib R, et al. Cycolobenzaprine for the treatment of myofascial pain in adults. Cochrane Database Syst Rev 2009;8:CD006830.
Huh J, Goebert D, Takeshita J, Lu BY, Kang M. Treatment of generalized anxiety disorder: A comprehensive review of the literature for psychopharmacologic alternatives to newer antidepressants and benzodiazepines. Prim Care Companion CNS Disord 2011;12(2):e1–9.
Lisi AJ, Breuer P, Gallagher RM, et al.
Deconstructing Chronic Low Back Pain in the Older Adult - Step by Step
Evidence and Expert-Based Recommendations for Evaluation and Treatment.
Part II: Myofascial Pain
Pain Medicine 2015 (Jul); 16 (7): 1282–1289Velly A, Gornitsky M, Philippe P. Contributing factors to chronic myofascial pain: A case-control study. Pain 2003;104:491–9
Faravelli C, Castellini G, Benni L, et al. Generalized anxiety disorder: Is there any specific symptom? Compr Psychiatry 2012;53:1056–62
Fernandez-de-las-Penas C, Dommerholt J. Myofascial trigger points: Peripheral or central phenomenon? Curr Rheumatol Rep 2014;16:395
Siu AL, Preventive Services Task Force US. Screening for depression in adults: US preventive services task force recommendation statement. J Am Med Assoc 2016;315(4):380–7

Return to LOW BACK PAIN
Since 8-30-2016
| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |