

Does Awareness of Key Reassuring Messages Influence
Patient Outcomes in Participants With Chronic Low
Back Pain? Secondary Analysis of an Observational
Study in Primary CareThis section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: European J Pain 2026 (Jul); 30 (6): e70306 ~ FULL TEXT
OPEN ACCESS Anika Young • Adrian Traeger • Simon French • Alice Kongsted
Mark Hancock • Inge Ris • Simon Kirkegaard • Hazel Jenkins
Department of Chiropractic,
Macquarie University,
Sydney, Australia.
Shavit ~ PLoS One 2025 (Sep 2)Background: Reassurance is recommended in the management of chronic low back pain (CLBP). Reassuring messages include that serious pathology has been excluded and movement is safe. The impact of patient awareness of reassuring messages on patient outcomes has not been investigated. We aimed to describe the characteristics of people reporting awareness of reassuring messages after a 3 month education and exercise program for CLBP and to determine if awareness of reassuring messages at 3 months influences patient outcomes at 6 months.
Methods: We performed a secondary analysis of 3850 adults who received a structured group-based education and exercise program for CLBP. Expert knowledge was used to construct directed acyclic graphs to identify relevant confounders. We used linear mixed models, adjusted for the identified confounders, to determine associations between self-reported awareness of reassuring messages at 3 months and patient outcomes at 6 months (pain, disability, fear-avoidance and self-efficacy), and to determine associations between baseline patient characteristics and awareness of reassuring messages at 3 months.
Results: More awareness of reassuring messages at 3 months positively influenced pain intensity (regression coefficients; 95% confidence interval: -0.27; -0.39, -0.14), disability (-1.01; -1.58, -0.44), and fear-avoidance (-0.85; -1.13, -0.57) at 6 months. Less threatening illness perceptions and higher levels of self-efficacy at baseline were associated with more awareness of reassuring messages at 3 months; whereas being older, male, having more leg pain, and higher fear-avoidance were associated with less awareness of reassuring messages at 3 months.
Conclusions: While effects were small, awareness of reassuring messages positively influenced patient outcomes at 6 months.
Significance statement: Our study is the first to examine whether patient awareness of reassuring messages influences patient outcomes in chronic low back pain. We found that more awareness of reassuring messages after a group education and exercise intervention reduced pain intensity, disability and fear-avoidance. While effects were small, awareness of reassuring messages positively influenced patient outcomes. Clinicians should consider the benefits of delivering key reassuring messages as part of multi-modal low back pain management.
From the FULL TEXT Article:
Introduction
Low back pain (LBP) is a highly prevalent condition, in 2020, LBP affected approximately 619 million people worldwide (Ferreira et al. 2023). While most people recover from an episode of LBP within 6 weeks, approximately 70% of people experience a recurrence within 12 months and up to 30% develop chronic low back pain (CLBP) (de Campos et al. 2023; Traeger et al. 2016). The 2024 World Health Organisation (WHO) guidelines recommend education and exercise therapy be used for the non-surgical management of CLBP (World Health Organisation 2023). Patient education is used to improve an individual's understanding of chronic pain, the contributing biopsychosocial factors, and to support them in developing strategies for self-management. Education may include providing a person with knowledge about diagnosis, help them make sense of their pain, dispel false/unhelpful beliefs such as risks associated with movement, assist with self-management strategies and pain-coping, and manage their expectations of recovery (Furlong et al. 2022; Moseley 2019; O'Sullivan et al. 2018). Exercise can improve function and reinforce reassuring messages by providing experiential reassurance about the safety of movement (Young, French, et al. 2025).
A person's beliefs about pain can contribute to their back pain outcomes (Corręa et al. 2022; Elfering et al. 2009; Grřn et al. 2019), and education is a mechanism to improve these beliefs (Buchbinder et al. 2001; George et al. 2009). Positive beliefs about back pain are associated with reductions in pain intensity (Grřn et al. 2019), compared to people who have more negative back pain beliefs, who experience delayed recovery (Elfering et al. 2009). As such, interventions that improve beliefs about pain would likely improve patient outcomes.
Despite beliefs about pain being (1) positively impacted by education and (2) associated with improved patient pain outcomes, patient education interventions have shown mixed effects on low back pain outcomes. For people with LBP, patient education has been shown in individual studies to reduce patient disability (Jenkins et al. 2025; Piano et al. 2025; Traeger et al. 2019), healthcare utilisation (Traeger et al. 2019), and fear (Traeger et al. 2015) and has favourable effects on return to work outcomes (Engers et al. 2008; Piano et al. 2022). However, systematic reviews investigating the effects of patient education have conflicting conclusions (Engers et al. 2008; Furlong et al. 2022; Jones et al. 2021; Piano et al. 2022, 2025). These contrasting conclusions likely arise from differences in the content, mode of delivery, duration and provider delivering the education, which in turn may provide a person with awareness of key educational messages to differing extents.
A person's awareness of key educational messages may be an important factor in determining a person's back pain outcomes after a course of education; however, data about peoples' awareness of reassuring educational messages are rarely collected in trials. GLA:D Back is a structured education and exercise program for people with CLBP. The key messages delivered as part of GLA:D Back include: the back is made for movement, the back is strong, the brain can turn pain up and down, pain is an alarm and does not equal harm, ‘bad’ posture is common, movements inhibit pain, exercise strengthens the back and action comes before improvement (Kjaer et al. 2018; Kongsted, Hartvigsen, et al. 2019). Such educational messages have been shown to be reassuring for people with back pain (Traeger et al. 2019) and will be referred to herein as ‘key reassuring messages’.
Aims
Our primary aim was to determine if awareness of key reassuring messages following a 3 month education and exercise program for CLBP influences clinical outcomes at 6 months (aim 1).
Our secondary aims were to describe the awareness of key reassuring messages among participants before and after entering an education and exercise program for CLBP (aim 2a), and to determine the characteristics of participants who report more awareness of key reassuring messages at 3 months (aim 2b).
Methods
Our protocol was pre-registered in Open Science Framework on the 7th of March 2025 (Young, Traeger, et al. 2025). Ethical approval was not required as determined by The Health Research Ethics Committee of Southern Denmark (file number S-20172000-93). The Danish Data Protection Agency (DPA) provided authorisation for data collection as part of the University of Southern Denmark's institutional authorisation (DPA no. 2015–57-0008 SDU no. 17/30591). Macquarie University Human Research Ethics Committee provided a waiver for this secondary analysis, as ethical standards were adhered to when conducting the study, and data were anonymised. Reporting of the manuscript adhered to the STROBE checklist (von Elm et al. 2008), see File S1.
Data Source
The data source was derived from the GLA:D Back program in Denmark (Kjaer et al. 2018; Kongsted, Ris, et al. 2019). GLA:D Back is a structured, group-based education and exercise intervention for people with chronic or recurrent low back pain conducted by GLA:D Back trained chiropractors or physiotherapists. Patients are eligible to participate in the GLA:D Back program if they have recurrent or persistent non-specific low back pain and are 18 years of age or over.
The educational component of the GLA:D Back program is delivered via two 1-hour group patient education sessions. The key messages from the education session are repeated during subsequent group exercise sessions, twice per week for 8 weeks. The educational component of the GLA:D Back program addresses the complexity of CLBP, including information on back pain epidemiology and biopsychosocial contributors, pain science, active coping strategies, and the importance of physical activity (Kjaer et al. 2018; Kongsted, Ris, et al. 2019).
All participants in the GLA:D Back program enter a clinical registry, with collection of patient-reported data for pain, function, disability, fear-avoidance, treatments sought, work, satisfaction and medication use. These data are collected via online questionnaires at baseline (prior to participation in the GLA:D Back program), then at 3 months, 6 months and 12 months after completing the GLA:D Back program.
Eligibility Criteria
To be included in this secondary analysis of data from the GLA:D Back clinical registry, participants must have received and completed the baseline questionnaire on or after the 15th May 2020, as questions related to key messages were added to the GLA:D Back online questionnaires on this date. In addition, to be considered eligible for aim 1, participants must have received the 6 month questionnaire, and to be considered eligible for aim 2b, participants must have received the 3 month questionnaire.
VariablesPatient Factors
Patient factors that may be associated with awareness of key reassuring messages were collected from patient participants at baseline before participating in the GLA:D Back program. These included sociodemographic factors (sex, age, education level), clinical factors (episode duration, back and leg pain intensity, disability, prognostic risk of LBP, self-efficacy, medication use), and psychological factors (fear-avoidance and brief illness perception questionnaire). Education level was categorised as either no education, further education (not university), university education, or other education. Episode duration was categorised as acute (< 4 weeks), sub-acute (4–12 weeks), or chronic (> 12 weeks). Back and leg pain intensity were measured using the numerical rating scale (NRS), scored from 0 to 10, where 0 is no pain and 10 is the worst pain imaginable (Jensen and McFarland 1993). Disability was measured using the Oswestry Disability Index (ODI), scored from 0 to 100 where lower scores indicate less disability and higher scores indicate more disability (Fairbank 1980). Prognostic risk was measured using the STaRT Back screening tool (STaRT Back), which was scored as low risk, medium risk, or high risk (Hill et al. 2008). Fear-Avoidance Beliefs Questionnaire physical activity (FABQpa) were scored from 0 to 24, with higher scores indicating higher levels of fear-avoidance due to LBP (Waddell et al. 1993). Beliefs were measured using the Brief Illness Perception Questionnaire (B-IPQ) sum score 0–80, where lower scores indicate a more threatening perception of the illness, and higher scores indicate a less threatening perception of the illness (Leysen et al. 2015). Symptom self-efficacy was assessed using the Arthritis Self-Efficacy Scale (ASES), scored from 0 to 50; higher scores indicate greater self-efficacy (Primdahl et al. 2010).
Awareness of Key Reassuring Messages

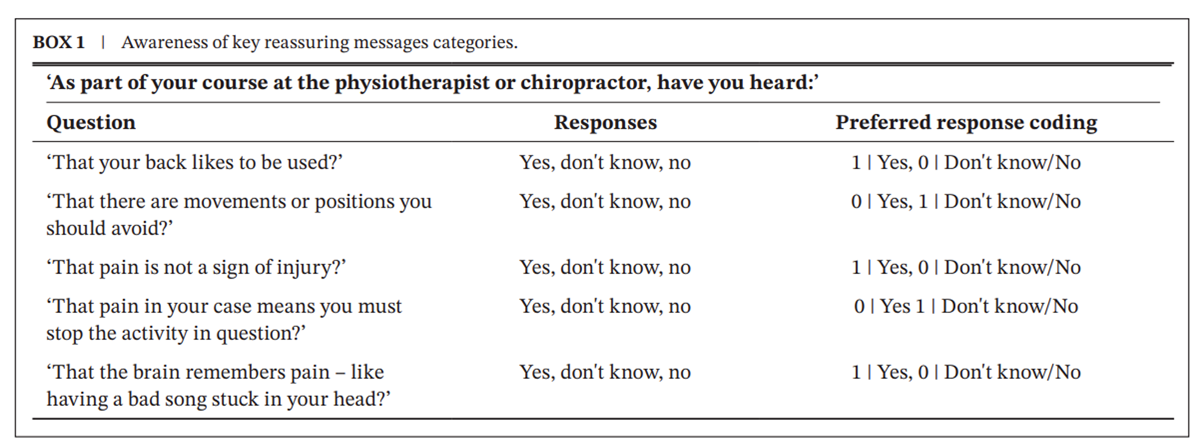
BOX 1 Participants were asked whether they were aware of the key reassuring messages before (baseline survey) and immediately after the conclusion of the GLA:D Back program (3 month survey). The five items were selected a priori to align with the key messages delivered in the GLA:D Back program. These questions are bespoke to reflect awareness of reassuring messages contained within the GLA:D Back program and have not been validated for use. Participants were asked if they had heard three messages that should have been delivered, and two messages that the program did not intend to deliver (Box 1), as these two questions were not generally considered helpful for understanding LBP and developing helpful pain behaviours.
Awareness of key reassuring message questions was coded based on whether participants responded with the preferred response or not. The data were collected for five key reassuring messages on a 3-point scale (yes, don't know, or no). We recoded the responses to the key messages as binary (yes or no), where ‘no’ equals both the ‘don't know’ and ‘no’ options. Box 1 explains the scoring for each key reassuring message. We also generated a reassurance sum score that ranged from 0 to 5, reflecting the number of preferred responses (having heard the three intended messages and not having heard the two non-intended messages), where lower scores indicate less awareness and higher scores indicate more awareness of reassuring messages.
Patient Outcomes at 6 Months
Patient outcomes were LBP intensity (NRS), disability (ODI), fear-avoidance (FABQpa), and self-efficacy (ASES) at 6 months. Fear-avoidance and self-efficacy were included as outcomes because these constructs may mediate improvements in pain and disability and are explicit treatment targets of the GLA:D Back program (Kjaer et al. 2018; Kongsted, Ris, et al. 2019).
AnalysesParticipant Demographics
We reported the baseline sociodemographic, clinical, and psychological features of the GLA:D Back participants stratified by groups: all participants and responders versus non-responders (at 3 and 6 months).
Effect of Awareness of Key Reassuring Messages at 3 Months on Patient Outcomes at 6 Months (Aim 1)
In a multivariable analysis with adjustment for potential confounders, we tested whether the reassurance sum score at 3 months influenced clinical outcomes at 6 months (pain intensity, disability, fear-avoidance, and self-efficacy). For pain, disability, fear-avoidance and self-efficacy, we used four different linear mixed models with random intercepts for clinics to account for the dependency of observations. We used expert knowledge from our multidisciplinary team to identify relevant confounders (Taylor et al. 2024). We have presented our assumptions using directed acyclic graphs (DAGs) constructed on DAGitty (Textor et al. 2016). The DAGs describing our hypotheses relating to the awareness of key messages (reassurance sum score) and patient outcomes are located in Files S2–S5.
For all 6 month patient outcomes, we adjusted for baseline age, sex, education, clinic, illness concern, pain intensity and reassurance sum score. For pain intensity at 6 months, we adjusted only for the aforementioned adjustment factors (File S2). For disability at 6 months, we adjusted for baseline disability in addition to the aforementioned adjustment factors (File S3). For fear-avoidance at 6 months, we adjusted for baseline fear-avoidance in addition to the aforementioned adjustment factors (File S4). For self-efficacy at 6 months, we adjusted for baseline self-efficacy and the aforementioned adjustment factors (File S5).
Participants' Awareness of Key Reassuring Messages Before and After an Education and Exercise Program for Chronic LBP (Aim 2a)
For aim 2a, we included all participants who had completed the baseline questionnaire. We calculated the proportion of participants who reported preferred responses to the awareness of each of the key reassuring messages at baseline (pre-GLA:D Back) and at 3 months (post-GLA:D Back). In addition, we reported the reassurance sum score (ranging from 0 to 5). We also reported the participant mean change scores in awareness from baseline to 3 months as well as the proportion of participants who had a positive change in awareness, no change in awareness, or a negative change in awareness.
Association Between Patient Characteristics at Baseline and Awareness of Key Reassuring Messages at 3 Months (Aim 2b)
We performed univariate and multivariable analyses to investigate the association between each patient factor and the reassurance sum score at 3 months (outcome variable). All patient factors described above were included in the analyses. All patient factors were retained in the multivariable models in accordance with our pre-specified protocol (Young, Traeger, et al. 2025). Selection of patient factors was guided by clinical expertise, rather than by statistical significance in univariate analyses. This ensured that important confounders were retained in the model, irrespective of univariate associations (Riley et al. 2019). We used linear mixed models with a random intercept for clinics to account for the dependency of observations. We controlled for participants' awareness of key reassuring messages at baseline (reassurance sum score).
We observed missingness and there is the likelihood that these data were not missing at random, or missing completely at random; therefore, imputation of missing values was not performed. For aims 1 and 2b, we tested for multicollinearity within the model by reviewing the variable inflation factor (VIF) and pairwise correlation coefficients. We planned to perform model reduction if any VIF was greater than 5, or the pairwise correlation coefficient was over 0.8 (Shrestha 2020; Vatcheva et al. 2016). All analyses were performed using STATA 18.0 (StataCorp 2023).
Results
Participant Characteristics
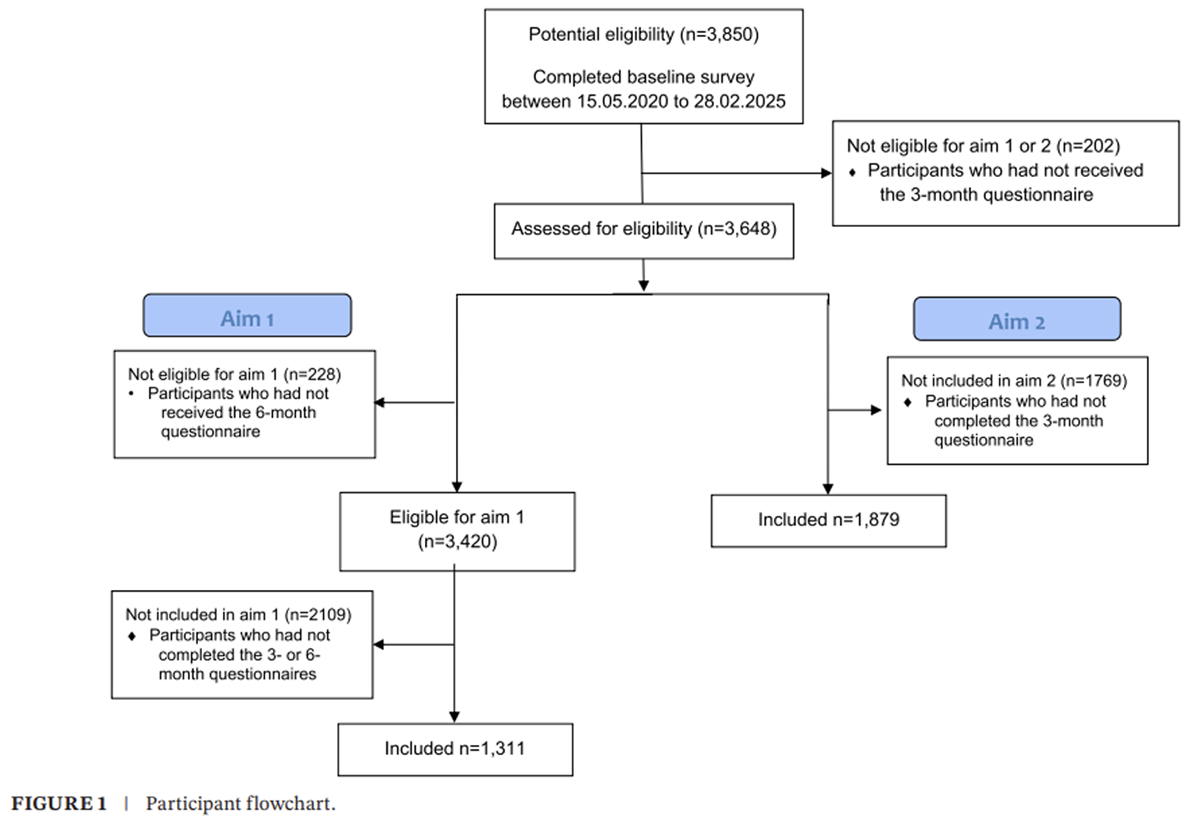
Figure 1 We identified 3850 potentially eligible participants from the GLA:D Back registry who had completed their baseline survey from 15.05.2020 to 28.02.2025. Of these, 3648 had received the 3 month questionnaire and were potentially eligible for either aim. For aim 1, 3420 participants who had also received the 6 month questionnaire were eligible to be included. Of these, 1311/3420 (38%) participants had responded to both the 3 month and 6 month questionnaires and were included in the analysis. For aim 2, 1879/3648 (52%) of participants had responded to the 3 month questionnaire and were included in the analysis. Figure 1 illustrates the selection of participants eligible for aims 1 and 2.
Table 1
page 6Table 1 compares the characteristics of all potentially eligible participants (n = 3850) to responders/non-responders to the 3 month and 6 month questionnaires. Characteristics were generally comparable across groups, except for some observable differences in participants' age, level of education, level of disability (ODI), prognostic risk (STaRT Back risk), and use of pain medicines. Non-responders tended to have lower rates of university education, higher disability scores, higher levels of prognostic risk and higher rates of pain medicine use.
Effect of Awareness of Key Reassuring Messages at
3 Months on Patient Outcomes at 6 Months (Aim 1)
More awareness of key reassuring messages at 3 months was associated with reduced pain intensity, disability and fear-avoidance at 6 months. For every additional message that a person was aware of at 3 months, there was a reduction on average of 0.27 points out of 10 on the back pain intensity scale (?0.27 points, 95% CI: ?0.39 to ?0.14), of 1.01 points out of 100 on the ODI scale (?1.01 points, 95% CI: ?1.58 to ?0.44), and of 0.85 points out of 24 on the FABQ-PA sub scale (?0.85 points, 95% CI: ?1.13 to ?0.57). Awareness of key reassuring messages at 3 months did not affect self-efficacy at 6 months (0.08 points, 95% CI: ?0.02 to 0.19).
Participants' Awareness of Key Reassuring Messages
Before and After an Education and Exercise Program
for Chronic LBP (Aim 2a)
At baseline, on average, participants had a reassurance sum score of 3.3 (SD 1.2), meaning that on average, 3.3 of the five key message questions were answered in the preferred direction (n = 2757) (Box 1). Awareness of the key reassuring messages increased at 3 months to 4.0 (SD: 1.00) of the 5 key reassuring messages (n = 1857). Overall, 1020 participants (57%) reported awareness of more key messages at 3 months, 510 participants (29%) had no change in awareness, and 249 participants (14%) reported less awareness of key messages.
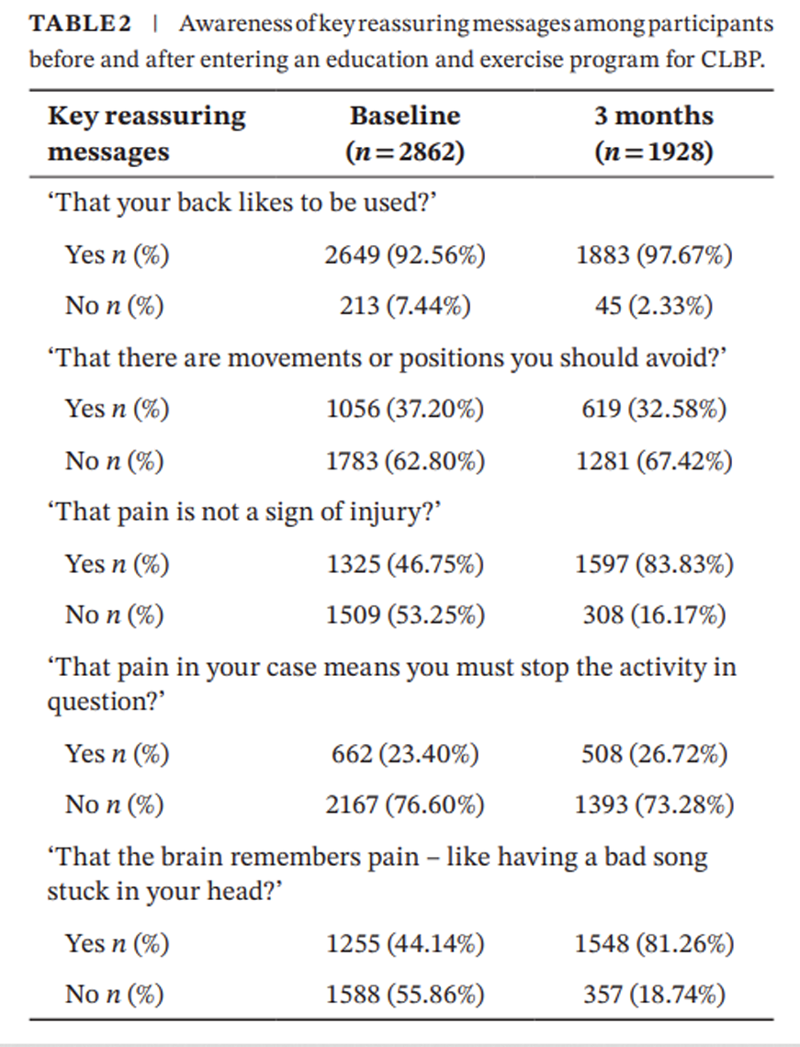
Table 2 The different proportions of participants who were aware of each individual key reassuring message at baseline and 3 months are presented in Table 2. Awareness of the key reassuring message ‘pain is not a sign of injury’ increased from 46.8% at baseline to 83.8% at 3 months; and ‘the brain remembers pain’ increased from 44.1% at baseline to 81.3% at 3 months. Approximately one third of participants were aware of the two messages that the program did not intend to deliver at baseline and there was no substantial change in awareness of these two messages at 3 months. ‘That there are movements or positions you should avoid?’ was recognised by 37.2% at baseline and 32.6% at 3 months; and ‘That pain in your case means you must stop the activity in question?’ by 23.4% at baseline and 26.7% at 3 months.
Associations Between Patient Characteristics at Baseline
and Awareness of Key Reassuring Messages
at 3 Months (Aim 2b)
Table 3
page 8Table 3 presents the univariate and multivariable model results. When accounting for patient factors in a multivariable model, less threatening illness perceptions and higher levels of self-efficacy at baseline were associated with more awareness of key reassuring messages at 3 months. For each point increase in the B-IPQ and ASES, there was, on average, a 0.01 (95% CI: +0.00 to 0.01) and 0.04 (95% CI: 0.01 to 0.07) between-person increase in the awareness of key reassuring messages sum score, respectively. In contrast, being older, male and having higher levels of leg pain and fear-avoidance were associated with less awareness of key reassuring messages at 3 months. For each year increase in age, there was on average a 0.01 (95% CI: ?0.01 to ?0.00) between-person reduction in awareness of key reassuring messages. Males scored on average 0.14 (95% CI: ?0.23 to ?0.04) points less in awareness of key reassuring messages when compared to females. For each 1-point increase on the leg pain numerical pain scale and the FABQ-PA, there was on average a 0.02 (95% CI: ?0.04 to ?0.00) and 0.02 (95% CI: ?0.03 to ?0.01) between-person reduction in awareness of key reassuring messages, respectively. Most variables had similar associations with the outcome in both univariate and multivariable models. However, in the multivariable model, associations were weakened for education, prognostic risk and disability, whereas a weak positive association was revealed for illness perceptions when compared to the univariate model.
Discussion
Key Findings
In this observational study of 1311 people with CLBP, more awareness of key reassuring messages at 3 months resulted in small improvements in pain intensity, disability and fear-avoidance, but not self-efficacy at 6 months. On average, participants reported awareness of more reassuring messages after an exercise and education program for chronic LBP. The increase in awareness was most notable for the key reassuring messages: ‘pain is not a sign of injury’ and ‘the brain remembers pain’. Having a less threatening perception of illness and self-efficacy at baseline was associated with more awareness of key reassuring messages at 3 months. Being older, male, having higher levels of leg pain and/or fear-avoidance were associated with less awareness of key reassuring messages at 3 months.
Comparison With Previous Literature
A person's awareness of key reassuring messages is a factor that influences patient outcomes. We found that more awareness of key reassuring messages after an education and exercise program improved patient outcomes, including pain, disability and fear-avoidance beliefs, compared to individuals with less awareness of key reassuring messages. Previous research investigating the role of patient beliefs on patient outcomes has similarly shown associations with pain, disability and back-pain related costs. As an example, a recent mediation analysis of a randomised controlled trial (276 participants) found that changing an individual's beliefs about the consequences of back pain, thus reducing catastrophic thoughts and fears about pain, reduced pain intensity and disability (Cashin et al. 2023). There is also research showing associations between reductions in fear-avoidance beliefs after a cognitive behavioural approach and reductions in disability for LBP (Fordham et al. 2017). On a population level, there is evidence that mass media educational campaigns about back pain can positively impact people's back pain beliefs and subsequently reduce disability and back pain-related costs (Buchbinder et al. 2001).
Reassurance may be associated with a person's intention to self-manage (O'Hagan et al. 2022), but increased awareness of reassuring messages did not appear to translate to increased self-efficacy. While we found no relationship between awareness of reassuring messages and self-efficacy, O'Hagan et al. (2022) found from observational data on 656 people with chronic LBP that people with positive attitudes towards educational messages about reassurance were more likely to intend to self-manage their LBP (O'Hagan et al. 2022). These findings highlight the complex relationship between reassurance, intention to self-manage and the effect on self-efficacy.
To our knowledge, this study is the first to investigate patient characteristics and their association with awareness of key reassuring messages after an education and exercise program for chronic LBP. While we cannot make direct comparisons to existing literature, a systematic review found that older, less educated, lower-income individuals and those with poorer self-rated general and mental health generally held more negative beliefs about back pain (Morton et al. 2019). Similarly, we found associations between older individuals and less awareness of key reassuring messages; however, these associations were small, and there is uncertainty regarding the clinical relevance of this association.
While clinical practice guidelines advise that education and advice should be delivered as first-line care for LBP management, there are scenarios when patients do not receive this. Observational data of healthcare providers demonstrate significant variability in the utilisation of education, where 20.5%–71.5% of people presenting for a consultation for LBP received education (Morsř et al. 2022; Williams et al. 2010). This highlights that there are still people who present to primary care who do not receive education. Clinicians should consider delivering reassuring messages, as they appear to positively impact patient LBP outcomes.
Strengths and Limitations
The strengths of our study were that the data we used were from a large and longitudinal sample. This is the first study to investigate the effects of awareness of key reassuring messages on patient outcomes. To ensure meaningful results for interpretation, we considered not only the strength of the associations but also reflected on the clinical relevance of the results.
While the findings provide novel insights, there are some limitations that may influence these results. A key limitation in this study is that the awareness of the key reassuring messages was used as a proxy, and it is unclear to what extent awareness reflects participants' understanding. In addition, these questions have not been validated. There was also a low response rate to the 3 and 6 month surveys. When comparing responders and non-responders (at both 3 and 6 months), some differences in characteristics were observed. Non-responders tended to have lower education, higher ODI scores, higher levels of high prognostic risk, and more use of pain medications. Lower educational attainment is associated with lower health literacy (Friis et al. 2016), and low health literacy is linked to poorer comprehension of health messages (Berkman et al. 2011). As a result, participants who were less able to understand the reassuring messages may have been disproportionately lost to follow-up, and participants with more favourable baseline profiles were potentially overrepresented in follow-up data. Therefore, attrition bias may have led to an over- or under-estimation of the associations observed. This study was observational, and every participant received the education and exercise intervention, meaning that there was no control group to assess how the intervention group compared to people who did not receive the intervention. While this design would be advantageous to appraise the effectiveness of the intervention, it does not answer which parts of the intervention are effective. We constructed DAGs to identify potential factors that could confound these relationships. In the analysis, we have not considered the fidelity of the participants or the clinics to the GLA:D Back program. While participants should have received these key reassuring messages as part of the GLA:D Back program, it is unknown whether the messages were delivered as intended. Further research has been conducted to develop a fidelity measure for clinicians delivering the GLA:D Back program (Heiberg et al. 2023). These results are based on analysis of the Danish GLA:D Back registry, and it is unclear whether these findings would be comparable in other countries.
Implications for Clinical Practice and Research
Our results demonstrated that more awareness of key reassuring messages positively influenced pain intensity, disability and fear-avoidance. While these improvements were small, we would not expect awareness of reassuring messages alone to be solely responsible for clinically important change. Instead, it likely plays a role as part of multi-modal management for LBP. Clinically important changes for pain intensity and disability have been defined in the literature (Ostelo and de Vet 2005). To contextualise our findings, for effects on pain and disability to be classified as achieving the minimally clinically important change, pain intensity on the NRS should reduce by > 2.5 out of 10 points (for persons with CLBP), and disability as scored by the ODI should reduce by > 10 out of 100 points (for LBP of any duration). Research has not yet established what the clinically important changes are for the FABQ (Swinkels-Meewisse et al. 2003).
While these improvements are unlikely to be clinically important alone, clinicians should consider the benefits of delivering key reassuring messages to people with CLBP. In addition, it is important to consider that the GLA:D Back program is multi-modal, including education and exercise delivered as a package of care. Combining education with other interventions is likely to enhance the effects on patient outcomes (World Health Organisation 2023). Therefore, healthcare providers should consider delivering these key reassuring messages to all people presenting with LBP. While the effects are small, patients who are aware of these messages demonstrated additional improvements, which may be worthwhile given that they are feasible to deliver and at low cost. Other options for dissemination of these messages could be a mass media campaign to increase the awareness of these key reassuring messages on a population level (Buchbinder et al. 2001).
There has been limited research that explores the role that a person's understanding and beliefs about pain play in improving patient health outcomes after an educational intervention for LBP. Future research should explore this relationship to determine how a person's understanding and beliefs about pain affect patient outcomes.
We found that awareness of reassuring messages influenced patient outcomes, and that older individuals, males, those with higher levels of leg pain or fear-avoidance were associated with slightly less awareness of key reassuring messages. Future research can explore whether these factors are consistent in different contexts and whether healthcare providers can enhance awareness of reassuring messages in these individuals.
Conclusions
More awareness of key reassuring messages at 3 months, after an education and exercise program, resulted in small improvements in pain intensity, disability and fear-avoidance at 6 months, but no improvement in self-efficacy. Less threatening illness perceptions and self-efficacy at baseline were associated with slightly more awareness of key reassuring messages at 3 months. Conversely, being older, male and having higher levels of leg pain and fear-avoidance were associated with slightly less awareness of key reassuring messages at 3 months.
Supporting Information
File S1 STROBE checklist.
File S2 Directed Acyclic Graph for awareness of key reassuring messages at 3 months and pain intensity at 6 months.
File S3 Directed Acyclic Graph for awareness of key reassuring messages at 3 months and disability at 6 months.
File S4 Directed Acyclic Graph for awareness of key reassuring messages at 3 months and fear-avoidance at 6 months.
File S5 Directed Acyclic Graph for awareness of key reassuring messages at 3 months and self-efficacy at 6 months.Author Contributions
Anika Young: conceptualisation, methodology, formal analysis, writing – original draft, writing – review and editing.
Adrian Traeger: conceptualisation, methodology, writing – review and editing and supervision.
Simon French: conceptualisation, methodology, writing – review and editing and supervision.
Alice Kongsted: conceptualisation, methodology, formal analysis and writing – review and editing.
Mark Hancock: conceptualisation, methodology and writing – review and editing.
Inge Ris: methodology and writing – review and editing.
Simon Kirkegaard: methodology and writing – review and editing.
Hazel Jenkins: conceptualisation, methodology, formal analysis, writing – review and editing and supervision.
Acknowledgements
Clinicians, patients for participation + OPEN (Open, Odense, Denmark) for access to REDCap. Open access publishing facilitated by Macquarie University, as part of the Wiley - Macquarie University agreement via the Council of Australasian University Librarians.
Funding
Anika Young received scholarship support from Macquarie University Pro Vice Chancellor's scholarship and funding from the Australia & New Zealand LBP Research Network.
Conflicts of Interest
The authors declare no conflicts of interest.
References:
Berkman, N. D., S. L. Sheridan, K. E. Donahue, D. J, et al. 2011.
Low Health Literacy and Health Outcomes: An Updated Systematic Review
Annals of Internal Medicine 155: 97–107.Buchbinder, R., D. Jolley, and M. Wyatt. 2001.
Population Based Intervention to Change Back Pain Beliefs and Disability: Three Part Evaluation
BMJ 322: 1516–1520.Cashin, A. G., H. Lee, B. M. Wand, et al. 2023
Mechanisms of Education and Graded Sensorimotor Retraining in People With Chronic Low Back Pain: A Mediation Analysis
Pain 164: 2792–2800.Corręa, L. A., S. Mathieson, N. A. M. Meziat-Filho, et al. 2022
Which Psychosocial Factors Are Related to Severe Pain and Functional Limitation in Patients With Low Back Pain?: Psychosocial Factors Related to Severe Low Back Pain
Brazilian Journal of Physical Therapy 26: 100413.de Campos, T. F., T. M. da Silva, C. G. Maher, N. C, et al. 2023
Prognosis of a New Episode of Low-Back Pain in a Community Inception Cohort
European Journal of Pain 27: 602–610.Elfering, A., A. F. Mannion, N. Jacobshagen, O. Tamcan, et al. 2009
Beliefs About Back Pain Predict the Recovery Rate Over 52 Consecutive Weeks
Scandinavian Journal of Work, Environment & Health 35: 437–445.Engers, A., P. Jellema, M. Wensing, D. A. van der Windt, et al. 2008
Individual Patient Education for Low Back Pain
Cochrane Database of Systematic Reviews 2008: Cd004057.Fairbank, J. 1980
The Oswestry Low Back Pain Disability Questionnaire
Physiotherapy 66, no. 8: 271–273.Ferreira, M. L., K. De Luca, L. M. Haile, et al. 2023
Global, regional, and national burden of low back pain,
1990–2020, its attributable risk factors, and
projections to 2050: a systematic analysis of
the Global Burden of Disease Study 2021
Lancet Rheumatol 2023 (May 22); 5 (6): e316-e329Fordham, B., C. Ji, Z. Hansen, R. Lall, and S. E. Lamb. 2017
Explaining How Cognitive Behavioral Approaches Work for Low Back Pain: Mediation Analysis of the Back Skills Training Trial
Spine 42: E1031–E1039.Friis, K., M. Lasgaard, G. Rowlands, R. H. Osborne, et al. 2016
Health Literacy Mediates the Relationship Between Educational Attainment and Health Behavior: A Danish Population-Based Study
Journal of Health Communication 21: 54–60.Furlong, B., H. Etchegary, K. Aubrey-Bassler, M. Swab, et al. 2022
Patient Education Materials for Non-Specific Low Back Pain and Sciatica: A Systematic Review and Meta-Analysis
PLoS One 17: e0274527.George, S. Z., D. S. Teyhen, S. S. Wu, et al. 2009
Psychosocial Education Improves Low Back Pain Beliefs: Results From a Cluster Randomized Clinical Trial (NCT00373009) in a Primary Prevention Setting
European Spine Journal 18: 1050–1058.Grřn, S., R. K. Jensen, T. S. Jensen, and A. Kongsted. 2019
Back Beliefs in Patients With Low Back Pain: A Primary Care Cohort Study
BMC Musculoskeletal Disorders 20: 578.Heiberg, B. D., I. Ris, H. H. Lauridsen, J. Hartvigsen, et al. 2023
The GLA: D BACK Self-Management Adherence and Competence Checklist (SMAC Checklist)—Development, Content Validity and Feasibility
British Journal of Health Psychology 28: 1052–1075.Hill, J. C., K. M. Dunn, M. Lewis, et al. 2008
A Primary Care Back Pain Screening Tool: Identifying
Patient Subgroups For Initial Treatment
(The STarT Back Screening Tool)
Arthritis Rheum. 2008 (May 15); 59 (5): 632–641Jenkins, H. J., L. Corręa, B. T. Brown, et al. 2025
Long-Term Effectiveness of Non-Surgical Interventions for Chronic Low Back Pain: A Systematic Review and Meta-Analysis
The Lancet Rheumatology 7, no. 9: e607–e617.Jensen, M. P., and C. A. McFarland. 1993
Increasing the Reliability and Validity of Pain Intensity Measurement in Chronic Pain Patients
Pain 55: 195–203.Jones, C. M. P., C. A. Shaheed, G. E. Ferreira, et al. 2021
Advice and Education Provide Small Short-Term Improvements in Pain and Disability in People With Non-Specific Spinal Pain: A Systematic Review
Journal of Physiotherapy 67: 263–270.Kjaer, P., A. Kongsted, I. Ris, et al. 2018
GLA:D() Back Group-Based Patient Education Integrated With Exercises to Support Self-Management of Back Pain—Development, Theories and Scientific Evidence
BMC Musculoskeletal Disorders 19: 418.Kongsted, A., J. Hartvigsen, E. Boyle, et al. 2019
GLA:D R Back: Group-Based Patient Education Integrated With Exercises to Support Self-Management of Persistent Back Pain—Feasibility of Implementing Standardised Care by a Course for Clinicians
Pilot and Feasibility Studies 5: 65.Kongsted, A., I. Ris, P. Kjaer, W. Vach, L. Morsř, et al. 2019
GLA:D Back: Implementation of Group-Based Patient Education Integrated With Exercises to Support Self-Management of Back Pain—Protocol for a Hybrid Effectiveness-Implementation Study
BMC Musculoskeletal Disorders 20: 85.Leysen, M., J. Nijs, M. Meeus, et al. 2015
Clinimetric Properties of Illness Perception Questionnaire Revised (IPQ-R) and Brief Illness Perception Questionnaire (Brief IPQ) in Patients With Musculoskeletal Disorders: A Systematic Review
Manual Therapy 20: 10–17.Morsř, L., J. Lykkegaard, M. K. Andersen, et al. 2022
Providing Information at the Initial Consultation to
Patients with Low Back Pain Across General Practice,
Chiropractic and Physiotherapy - A Cross-sectorial
Study of Danish Primary Care
Scand J Prim Health Care 2022 (Oct 31); 1–9Morton, L., M. de Bruin, M. Krajewska, D. Whibley, et al. 2019
Beliefs About Back Pain and Pain Management Behaviours, and Their Associations in the General Population: A Systematic Review
European Journal of Pain 23: 15–30.Moseley, G. L. 2019
Whole of Community Pain Education for Back Pain. Why Does First-Line Care Get Almost no Attention and What Exactly Are We Waiting for?
British Journal of Sports Medicine 53, no. 10: 588–589.O'Hagan, E. T., F. Di Pietro, A. C. Traeger, et al. 2022
What Messages Predict Intention to Self-Manage Low Back Pain? A Study of Attitudes Towards Patient Education
Pain 163: 1489–1496.Ostelo, R. W., and H. C. de Vet. 2005
Clinically Important Outcomes in Low Back Pain
Best Practice & Research. Clinical Rheumatology 19: 593–607.O'Sullivan, P. B., J. P. Caneiro, M. O'Keeffe, et al. 2018
Cognitive Functional Therapy: An Integrated Behavioral Approach for the Targeted Management of Disabling Low Back Pain
Physical Therapy & Rehabilitation Journal 98: 408–423.Piano, L., P. Audasso, L. Benzi, et al. 2025
Individual Education for Patients With Chronic Low Back Pain: Likely a Clinically Relevant Effect for Long-Term Disability Compared to Noneducational Interventions. A Systematic Review With Meta-Analysis
Journal of Orthopaedic & Sports Physical Therapy 55: 331–343.Piano, L., V. Ritorto, I. Vigna, M. Trucco, H. Lee, et al. 2022
Individual Patient Education for Managing Acute and/or Subacute Low Back Pain: Little Additional Benefit for Pain and Function Compared to Placebo. A Systematic Review With Meta-Analysis of Randomized Controlled Trials
Journal of Orthopaedic & Sports Physical Therapy 52: 432–445.Primdahl, J., L. Wagner, and K. Hřrslev-Petersen. 2010
Self-Efficacy in Rheumatoid Arthritis: Translation and Test of Validity, Reliability and Sensitivity of the Danish Version of the Rheumatoid Arthritis Self-Efficacy Questionnaire (RASE)
Musculoskeletal Care 8: 123–135.Riley, R. D., K. I. Snell, K. G. Moons, and T. P. Debray. 2019
Ten Principles to Strengthen Prognosis Research
In Prognosis Research in Healthcare: Concepts, Methods, and Impact.
Oxford University Press.Shrestha, N. 2020
Detecting Multicollinearity in Regression Analysis.
American Journal of Applied Mathematics and Statistics 8: 39–42.StataCorp. 2023.
Stata Statistical Software: Version 18. StataCorp LLC.Swinkels-Meewisse, E. J., R. A. Swinkels, A. L, et al. 2003
Psychometric Properties of the Tampa Scale for Kinesiophobia and the Fear-Avoidance Beliefs Questionnaire in Acute Low Back Pain
Manual Therapy 8: 29–36.Taylor, H., H. Crabbe, C. Humphreys, et al. 2024
Development and Use of a Directed Acyclic Graph (DAG) for Conceptual Framework and Study Protocol Development Exploring Relationships Between Dwelling Characteristics and Household Transmission of COVID-19—England, 2020
Building and Environment 250: 111145.Textor, J., B. van der Zander, M. S. Gilthorpe, M, et al. 2016
Robust Causal Inference Using Directed Acyclic Graphs: The R Package ‘Dagitty’
International Journal of Epidemiology 45: 1887–1894.Traeger, A. C., N. Henschke, M. Hübscher, et al. 2016
Estimating the Risk of Chronic Pain: Development
and Validation of a Prognostic Model (PICKUP)
for Patients with Acute Low Back Pain
PLoS Med. 2016 (May 17); 13 (5): e1002019Traeger, A. C., M. Hübscher, N. Henschke, G. L, et al. 2015
Effect of Primary Care-Based Education on Reassurance in Patients With Acute Low Back Pain: Systematic Review and Meta-Analysis
JAMA Internal Medicine 175: 733–743.Traeger, A. C., H. Lee, M. Hübscher, et al. 2019
Effect of Intensive Patient Education vs Placebo
Patient Education on Outcomes in Patients With
Acute Low Back Pain: A Randomized Clinical Trial
JAMA Neurol 2019 (Feb 1); 76 (2): 161–169Vatcheva, K. P., M. Lee, J. B. McCormick, and M. H. Rahbar. 2016
Multicollinearity in Regression Analyses Conducted in Epidemiologic Studies
Epidemiology (Sunnyvale) 6: 227.von Elm, E., D. G. Altman, M. Egger, S. J. Pocock, P. C, et al. 2008
The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for Reporting Observational Studies
Journal of Clinical Epidemiology 61: 344–349.Waddell, G., M. Newton, I. Henderson, D. Somerville, and C. J. Main. 1993
A Fear-Avoidance Beliefs Questionnaire (FABQ) and the Role of Fear-Avoidance Beliefs in Chronic Low Back Pain and Disability
Pain 52: 157–168.Williams, C. M., C. G. Maher, M. J. Hancock, et al. 2010
Low Back Pain and Best Practice Care:
A Survey of General Practice Physicians
Archives of Internal Medicine 2010 (Feb 8); 170 (3): 271–277World Health Organisation. 2023
WHO Guideline for Non-Surgical Management of Chronic Primary
Low Back Pain in Adults in Primary and Community Care SettingsYoung, A., S. D. French, A. C. Traeger, J. Ayre, et al. 2025
Clinician Experiences in Providing Reassurance for
Patients with Low Back Pain in Primary Care:
a Qualitative Study
J Physiotherapy 2025 (Jan); 71 (1): 48ń56Young, A., A. Traeger, S. French, et al. 2025
Does Awareness of Key Reassuring Messages Influence Clinical Outcomes in People With Chronic Low Back Pain?
https://doi.org/10.17605/OSF.IO/SR4W7.
Return to LOW BACK PAIN
Since 6-12-2026
| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |