

Efficacy of Spinal Manipulative Therapy in Older Adults
with Chronic Spinal Conditions:
An Updated Systematic ReviewThis section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: J Canadian Chiropractic Association 2026 (Apr); 70 (1): 27–54 ~ FULL TEXT
OPEN ACCESS Alec L. Schielke, DC • Robert J. Trager, DC • Joel M. Stevans, DC, PhD • Morgan R. Price, DC
Ronald D. Wilcox, DC • Sheryl A. Walters, MLS • Clinton J. Daniels, DC, MS
Integrated Primary Care,
VA Palo Alto Health Care System,
Palo Alto, CA, USA.
Background: This systematic review evaluated the efficacy of SMT for chronic spinal conditions in adults aged 55 years and older.
Methods: We searched multiple databases for randomized controlled trials (RCTs) on SMT for older adults with chronic spinal conditions (≥ 12 weeks) published from February 2016 through October 2024. Additionally, studies from the prior article being updated were included as appropriate. Eligible studies compared SMT to active or inert comparators, measuring pain, function, or quality of life.
Results: Nine reports were included, evaluating SMT for chronic low back pain (5 RCTs, n=544), chronic neck pain (2 RCTs, n=241), lumbar spinal stenosis (1 RCT, n=259), and combined neck/back disability (1 RCT, n=182).
Conclusion: SMT may offer comparable or modestly greater benefit than other treatments for chronic spinal conditions in older adults, particularly for neck pain and LSS. Evidence certainty remains very low to moderate.
Registration: PROSPERO (CDR42024615084).
Keywords: musculoskeletal manipulations; aged; chiropractic; chronic pain; low back pain; lumbar spinal stenosis; neck pain; older adults; spinal manipulation.
From the FULL TEXT Article:
Introduction
Low back pain (LBP) is the leading cause of years lived with disability globally, with prevalence and disability increasing with age, peaking from ages 80 to 84 years. [1] Neck pain (NP) is ranked 11th in terms of years lived with disability globally, having a peak prevalence between age 50 and 74. [2] Despite these conditions being highly prevalent, there remain limitations in the evidence for efficacious treatments in older adults. [1, 2] In general, older adults exhibit a slower recovery from new episodes of back pain, and have a greater tendency to develop chronic symptoms. [3] Compared to younger adults, older adults are more likely to be severely debilitated by LBP, have decreased mobility, reduced independence, and require greater healthcare needs. [4]
Although chiropractic services are used less by older patients (≥55 years) compared to the general population, [5] at least 20% of chiropractic patients are older adults. [6] Non-surgical, non-pharmacologic interventions such as spinal manipulative therapy (SMT), massage, and exercise, are recommended as first-line approaches to care for LBP. [7–9] SMT is a treatment offered by chiropractors, physical therapists with advanced training, and some osteopaths and may be appropriate for older adults with chronic spine pain. Several observational studies have reported that SMT for older adults with spine pain is associated with reductions in cost and escalation of health care service utilization (e.g. imaging, injections, surgeries). [10–12] Best practices guidelines for the chiropractic management of older adults have been available since 2010, [13] with a subsequent update in 2017. [14] However, there are notable gaps in high quality evidence syntheses evaluating the efficacy of SMT derived from randomized controlled trials (RCTs) in older adults. [15]
Over the past decade, two systematic reviews on the topic of SMT for older adults have been conducted. Hawk et al. (2017) conducted a systematic review, which was used alongside a Delphi process to create best practices statements for chiropractors caring for older adults. [14] Hawk et al. identified six efficacy or effectiveness studies and concluded that there were evidence gaps regarding SMT in older adults, with current best practice recommendations being supported by expert opinion. Jenks et al. (2022) conducted an individual participant data meta-analysis including 10 studies with 786 patients total, with a search date ending in 2020. [16]
The meta-analysis found that SMT provided similar outcomes to recommended interventions for pain and functional disability in the older adult with chronic LBP, ultimately supporting SMT as an intervention. Despite these promising findings, evidence synthesis is needed for conditions beyond LBP, including stenosis with claudication, and NP. An updated literature synthesis is also needed to capture potential growth in the scientific literature.
Considering potential growth in available evidence since these previously reported systematic reviews on this topic, there is a need for an updated review on the topic of efficacy of SMT in older adults with chronic spinal conditions. The purpose of this systemic review was to investigate the efficacy of SMT for chronic spinal conditions in older adults. This study is an update of Hawk et al.’s 2017 systematic review performed as part of best practice consensus publication. [14] In contrast to the prior update, this review does not include any best practices nor guideline component. However, our results will provide evidence on SMT research to inform a separate clinical practice guideline update for the chiropractic management of older adult patients.
Methods
Registration and protocol
The study protocol was prospectively registered with the International Prospective Register of Systematic Reviews (PROSPERO) in November 2024 (CDR42024615084). Our reporting adheres to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA-2020). [17]
Eligibility criteria
To evaluate the efficacy of SMT for chronic spinal conditions in older adults, we translated PICOS elements (Population, Intervention, Comparison, Outcome, and Study Type) into eligibility criteria.
Population
We included studies in which the study population had a mean or median age of 65 years or older, or the minimum age for study inclusion was 55 years, to ensure generalizability to an older adult population. Chronic spinal conditions were defined as those persisting for a minimum duration of 12 weeks. We chose an age threshold to ensure generalizability to an older adult population while allowing inclusion of relevant studies. This decision was made a priori in consultation with the co-author team, considering the variable age definitions of “older adults” used in prior research studies, clinical guidelines, policy documents, and international literature. [18, 19]
Several factors supported our choice:(1) our review updates a prior systematic review [14] that included an RCT enrolling participants aged ≥55 years, [20] and we aimed to retain this study for consistency;
(2) we aimed to maximize the number of eligible studies;
(3) age-related changes to the spine often begin before age 65 and may influence response to SMT; [21]
(4) the American Geriatrics Society [22] allows for inclusion of studies with a median age over 65 years, even when some participants are younger; and
(5) SMT delivery may be modified for patients in their late 50s or early 60s due to age-related changes, for example reductions in bone density, [23] making this group clinically relevant to our review.Intervention
The intervention of interest was SMT, defined broadly as manual therapy of the spinal vertebral joints, excluding soft tissue techniques such as massage. More specifically, SMT was defined as both high-velocity low-amplitude (HVLA) techniques and low-velocity low-amplitude techniques applied to the spine. This refers to both manual treatments and mechanically assisted treatment (e.g., instrument techniques, flexion-distraction, drop table). SMT could include any portion of the vertebral column, including the occipital-cervical junction, cervical, thoracic, lumbar, and pelvic regions, including the sacroiliac joints.
SMT must have been performed by a licensed health care professional (e.g., chiropractor, physical therapist, osteopath). Other non-pharmacological, non-surgical interventions could be provided in conjunction with SMT. These could include but were not limited to, mind-body interventions, acupuncture, massage therapy, acupressure, electrical modalities, heat or cold, or other manual therapies.
Comparators
Comparison groups could include any active pharmacologic or non-pharmacologic intervention, placebo/sham interventions, waitlist controls, or no treatment. This broad inclusion maximized our ability to draw inferences from the available literature.
Outcomes
The primary outcomes assessed were pain intensity, physical function, quality of life, and activities of daily living. Secondary outcomes included markers of health service utilization such as surgery, medication, and medical visits when reported among included studies.
Study type

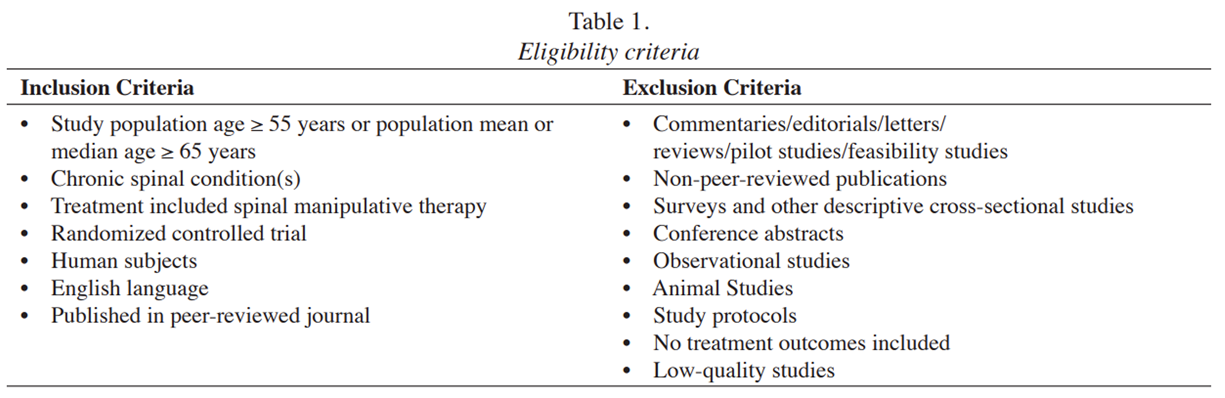
Table 1 We considered RCTs published in peer-reviewed journals in English. We excluded commentaries, editorials, letters, reviews, pilot or feasibility studies, non-peer-reviewed publications, surveys, observational studies, conference abstracts, animal studies, study protocols, and studies lacking treatment outcomes. The eligibility criteria are reported in Table 1.
Information sources
This study included RCTs from Hawk et al.’s 2017 systematic review performed on the same topic. [14] Given methodological revisions to expand on the age range of inclusion, restriction to chronic pain conditions, and focus on clinical trials, the three RCTs included in the previous review were all re-screened for eligibility in this update. Our database searches included PubMed, Cochrane Central Register of Controlled Trials, Cumulative Index to Nursing and Allied Health Literature (CINAHL), Allied and Complementary Medicine Database (AMED), Index to Chiropractic Literature, and Physiotherapy Evidence Database (PEDro). The search for Index for Chiropractic Literature was conducted on October 28, 2024, and all other searches were conducted on October 30, 2024. Gray literature searches included citation tracking of included articles, and consulting topic experts in search of relevant articles, which was performed on December 2, 2024.
Search strategy
The search strategy was developed in collaboration with a health sciences librarian (SW). A second health sciences librarian evaluated the comprehensiveness of the search strategy using the Peer Review of Electronic Search Strategies (PRESS) [24] checklist. Searches were limited to academic journals and the English language. Search terms were relevant to older adults, chronic musculoskeletal spinal conditions, and manipulation or manual therapy. The search was limited by publication date from February 1, 2016 (following the Hawk et al. search end date) through October 2024. As an example, the PubMed search syntaxes can be found in Appendix 1.
Selection process
Retrieved citations were uploaded to a Zotero25 library and then the Rayyan [26] online systematic review software. Two reviewers (MP and RW) independently screened titles and abstracts for eligibility and resolved disagreements by discussion. The same two reviewers then performed full-text screening. Disagreements were resolved by discussion between the reviewers, and when needed, a third investigator (AS) assisted until consensus was achieved. In cases where multiple articles were derived from the same RCT, we included secondary reports only when they presented unique outcomes or analyses not available in the primary publication.
This included data on responder outcomes, healthcare utilization, or cost-effectiveness. Accordingly, this strategy avoided duplication of primary outcomes such as pain and physical function and allowed us to capture a broader range of outcomes relevant to our aims. All included reports were linked to their respective primary RCTs and reported transparently in the data extraction tables. Considering our non-meta-analytic, qualitative approach and broad scope, inclusion of these secondary analyses provided additional data to support evidence synthesis.
Data collection process
Data extraction of the included RCTs was completed independently by two investigators (RT and JS). A third investigator (AS) verified the data, with discussion to resolve discrepancies. Extracted data were entered into a pre-designed Microsoft Excel worksheet. Corresponding authors of two of the included RCTs were contacted for additional information and clarifications,27,28 which were provided by one author. [27]
Data items
Information collected for each study included the first author’s surname, year of publication, sample size, patient age, symptom duration, condition(s)/diagnosis, treatment/intervention groups, sample size at allocation, and description of any group(s) with SMT, intervention group(s) dosage, comparison groups, sample size at allocation, and description of any group(s) without SMT, comparison group(s) dosage, follow-up duration for primary outcomes, pain and disability outcome measures, between-group effect estimate(s) for primary outcomes, responder analysis for within-group differences (if reported/calculated), other health service outcomes, between-group effect estimate(s) for other health service outcomes (if reported/calculated), and a summary of the key findings. We avoided specific requirements for follow-up durations among included studies. Instead, our strategy aimed to include all relevant outcomes reported, emphasizing any study-defined primary outcomes in our analysis. This ostensibly allowed us to capture the range of available evidence given the limited expected number of eligible studies.
For each RCT, we extracted means, standard deviations and confidence intervals (CIs) from the tables, text, or figures, as available. For two studies that did not provide between-group mean differences, [27, 29] the values were calculated with assistance from a statistician. For one study, which did not provide standard deviations (SD), [29] differences were imputed using pooled variance for Oswestry Disability Index (ODI), 36-Item Short Form Survey (SF-36), and Visual Analog Scale (VAS), using the Satterthwaite approximation to calculate degrees of freedom for each. [30] For the other study, [27] we calculated the mean difference in post-treatment pain scores and SDs and used the t-statistic to derive the 95% confidence intervals. [31]
Study risk of bias assessment
Included RCTs were evaluated independently by two investigators (RT and JS) using the Scottish Intercollegiate Guideline Network (SIGN) checklist. [32] Several tools are available to assess the quality and risk of bias of RCTs, including the Cochrane Risk of Bias tools (RoB 1 and RoB 2), the SIGN checklist, tools from the Joanna Briggs Institute, and others. We opted to use the SIGN checklist as it is a practical, straightforward, and validated tool. [33] Each SIGN question was assigned a value of “1” for each “yes” response and a value of “0” for “no” or “not applicable.”
Disagreements were resolved by including additional reviewers (AS and CD) and discussion until a consensus was reached. The SIGN tool also allows raters to enter free-text comments to support their individual scores, which facilitated discussion and resolution of discrepant scores. The SIGN checklists provided each study with a raw score from 0–10, with single-site trials being scored out of a total of nine points, instead of ten, because one question was only relevant to multisite trials. [32, 34]
These raw scores were then divided by the total sum of scores across the total of applicable domains and multiplied by 100 to make a percentage scoring system. We operationalized scoring thresholds in alignment with risk of bias assessments and corresponding quality, a strategy which has been used previously for risk of bias assessment. [35–38] We interpreted scores of ≥80% as being “high quality, low risk of bias,” 50% to 79% as “acceptable quality, moderate risk of bias,” and <50% as “low quality, high risk of bias.” For reports of secondary analyses, we evaluated the risk of bias based on their primary RCT. For the SIGN checklist we adapted item four regarding blinding to interpret it in respect to blinding of the outcome to the assessors, rather than clinicians delivering SMT or SMT recipients, to provide a more realistic and practical assessment of RCTs focused on SMT. [39]
Effect measures
We reported mean differences between groups along with confidence intervals and P-values for primary outcomes. Secondary outcomes, when present, included odds ratios or proportions of patients reaching improvement thresholds.
Synthesis methods
We qualitatively synthesized the extracted data from the included studies. We assessed clinical heterogeneity by comparing study characteristics, including patient population characteristics, condition treated, SMT co-interventions, comparator interventions, outcome measures, and duration of follow-up.
After reviewing previous literature reviews on the topic, [14, 16] our team decided a priori to avoid meta-analysis. First, we expected only a small number of studies would meet our inclusion criteria, limiting the ability to pool data meaningfully. Second, the total sample size across eligible studies was expected to be low (e.g., <400 participants), increasing the potential for imprecision. [40] Third, we anticipated clinical heterogeneity across studies from variations in patient populations (e.g., age, baseline symptoms), SMT protocols (e.g., technique, frequency), comparators (e.g., exercise, sham), and outcome measures (e.g., pain scales, functional status tools) which would hinder analysis.
Reporting bias
To assess potential reporting bias, one investigator (CD) extracted funding sources from included articles and searched ClinicalTrials.gov in February 2025. [42] Funding sources were categorized as either industry or non-industry, [42] and the Clinical Trials database was searched to identify whether any potentially eligible clinical studies had not been published. [43]
Certainty assessment
We utilized the GRADE (Grading of Recommendations Assessment, Development, and Evaluation) [40, 44–48] system to assess the overall quality of the evidence. Two investigators (AS and CD) performed GRADE assessments independently. When there were disagreements, additional investigators (RT and JS) were included and discussed the ratings until consensus was achieved. Outcomes were automatically deemed “very low” certainty if no trials were identified that reported on that given outcome.
Results
Study selection
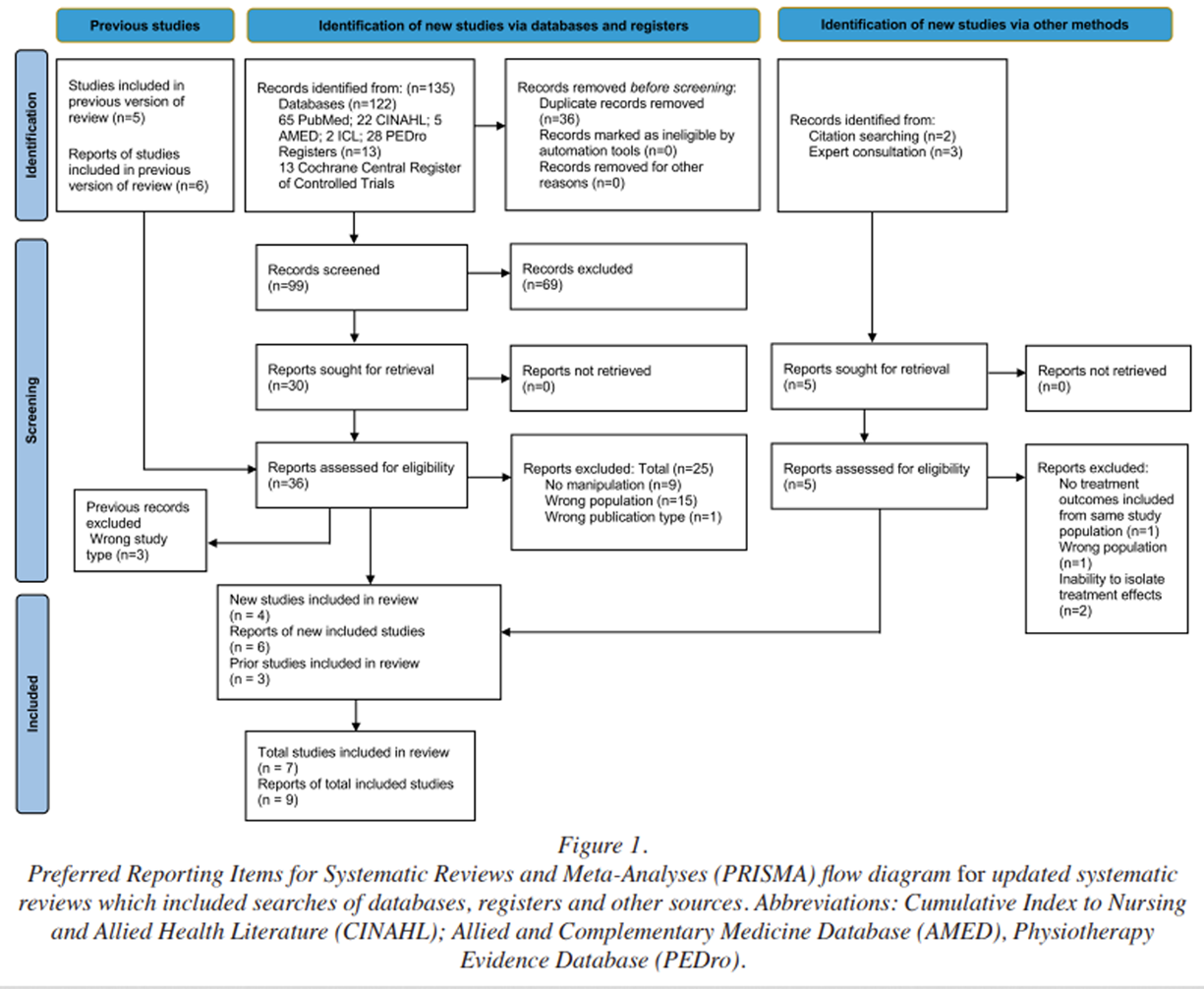
Figure 1 The search yielded 99 unique citations, and after title and abstract screening, 30 studies were potentially relevant, and the full-text reports were retrieved for assessment (Figure 1). Percentage agreement was 73% for title and abstract screening, and 100% for full-text screening. Five full-text records were identified through reference tracking and expert consultation, and an additional six reports (five studies) from the 2017 Hawk et al. study brought the total number of full-texts to be screened to 38; of those, 32 were excluded (reasons for exclusion detailed in Appendix 2). [49–80]
A total of six new reports (four studies, [28, 81–83] and two secondary analyses [84, 85] ) were included as a result of the updated database search, in combination with three studies [20, 27, 29] from the prior 2017 Hawk et al. systematic review, resulting in a total of nine reports [20, 27–29, 81–85] of seven RCTs [20, 27–29, 81–83] included in this systematic review.
Study characteristics
Five studies reported on LBP,20,27–29,85 two reported on NP,81,84 one reported on both NP and LBP,82 and one reported on LSS.83 Regarding the studies reporting on chronic LBP intervention and comparison group: Learman et al. compared thrust manipulation plus a home exercise program to non-thrust manipulation plus a home exercise program (standing hamstring stretches, cat and camel, quadruped pelvic rocking, prone press-ups, and supine lying piriformis stretches); Dougherty et al. compared SMT to sham treatment (detuned ultrasound); Enix et al. compared SMT plus soft tissue manipulation (proprioceptive neuromuscular facilitation stretching, post-isometric exercise relaxation techniques, transverse friction massage, and passive stretching) to multimodal physical therapy exercise (neuromuscular re-education, muscle endurance and strength training exercises, flexibility stretches, interferential electrical stimulation, ultrasound, postural education, and home exercise program); and Schulz et al. compared three groups, which were SMT (including up to four minutes of adjunct therapies to facilitate SMT) plus home exercise program (self-care for pain, low load exercises with graded progressions, stretching exercises muscle strength and endurance exercises, and balance exercises), supervised exercise program (self-care for pain, light aerobic warm up on stationary equipment, low load exercise, stretching, strength and balance exercises as described for home exercise program,) plus home exercise program, and home exercise program alone.
Maiers et al. (2014) reported on chronic NP comparing three groups: SMT plus home exercise and advice (information regarding pain management, consistent messaging to stay active, daily prescribed exercise to improve flexibility, balance, and coordination, as well as enhance trunk strength and endurance); supervised exercise program plus (one hour session high repetitions of low load exercises with the aim of increasing flexibility, endurance, strength, and balance) home exercise and advice; and home exercise and advice alone.
Maiers et al. (2019) reported on both chronic NP and chronic LBP and compared treatment duration of SMT plus supervised exercises (aerobic warm up and standardized program of stretching, strengthening, and balance exercises) for 12 weeks versus 36 weeks. Schneider et al. reported on LSS and compared three groups which were medical care (oral medication or epidural steroid injections as indicated), group-based exercise (supervised exercise classes for older adults), as well as manual therapy (including lumbar distraction mobilization, and lumbar/sacroiliac joint mobilization) and individualized exercises.
Leininger et al. published a secondary analysis of the Maiers et al. (2014) RCT to investigate between group cost-effectiveness, and Maiers et al. (2021) published a secondary analysis of Maiers et al. (2019) to investigate baseline factors related to response and outcomes for LBP and disability.
Table 2 Table 2 summarizes study characteristics. In total, 1,226 patients were included across all studies, with 579 patients receiving SMT. Mean patient ages varied from 64.5 years to 74.7 years, with the youngest and oldest individual ages reported to be 55 and 94 years, respectively. The number of patients and RCTs per condition were most for LBP with five RCTs including 544 unique patients total, with other conditions only having one RCT and fewer patients (LSS: n=259; NP: n=241; NP and disability and LBP and disability n=182). Symptom duration ranged from >12 weeks to 13.7 years.
Follow-up duration for primary outcomes ranged from five weeks to 36 weeks. Accordingly, the maximum durations of follow-up included in the analysis spanned Cochrane-defined windows of short term (closer to four weeks) to intermediate-term (closer to six months) and are reported in Table 2.86 The most common outcome measures for pain and disability were the ODI (n=3 RCTs), SF-36 (n=3 RCTs), Neck Disability Index (NDI) (n=2 RCTs), and 11-Box Pain Scale (n=3 RCTs).
Additional primary outcome measures, included in only one RCT, were the Numeric Pain Rating Scale (NPRS), VAS, 21-point Box Scale (pain), Modified Roland Scale (MRS), EuroQol EQ-5D (EQ), Short Physical Performance Battery (SPPB), Swiss Spinal Stenosis Questionnaire (SSS), and Self-Paced Walking Test (SPWT).
Risk of bias in studies
Table 3
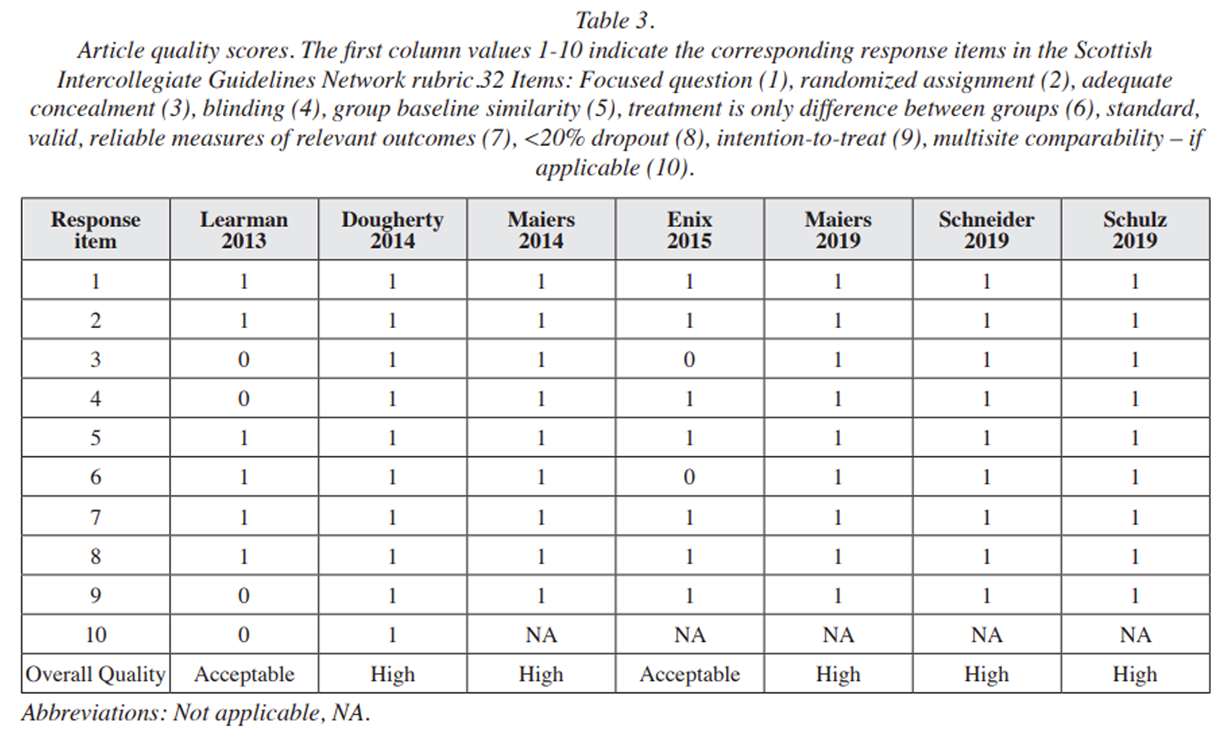
Table 4 Table 3 lists the risk of bias of the seven included RCTs. Five studies were assessed as high-quality (low risk of bias), [28, 29, 81–83] and two were acceptable quality (moderate risk of bias). [20, 27] No studies were assessed as low quality (high risk of bias).
Results of individual studies
Individual study results are available in Table 4., as well as a responder analysis table and health services outcomes table in the Appendix 3 and Appendix 4, respectively.
Results of synthesesLow back pain
Across three RCTs, [27–29 ] SMT showed no significant between-group difference between active or inert comparators for pain measures for LBP. Regarding low back-specific disability, one RCT found a statistically significant but not clinically meaningful benefit favoring SMT over an inert comparator, [29] while another RCT using an active exercise comparator found results favoring the null. [28] Two RCTs found no significant between-group difference in disability or functional status for LBP. [28, 29]
Two RCTs evaluated the comparative efficacy of SMT treatment parameters for LBP and disability. [20, 82] Learman et al. found no significant difference between thrust and non-thrust SMT, while Maiers et al. (2019) reported no significant difference related to SMT treatment duration (i.e., 12 weeks versus 36 weeks).
Schulz et al. explored responder analyses, noting modest differences favoring SMT at 12 weeks (16% more participants experienced a 30%–49% pain severity reduction [i.e., moderate], and 18% more participants with a 50% or greater [i.e., substantial] pain reduction), [87] although most responder outcomes were similar between groups. Schulz et al. and Maiers et al. (2019) reported no significant between-group differences with respect to medication use. A secondary analysis found that among older adults with back disability, a longer duration of symptoms greater than 14.5 years predicted a poorer response to SMT and exercise. [85]
Lumbar spinal stenosis
One RCT evaluated the efficacy of SMT with individualized exercise for LSS. [83] The SMT group yielded greater reductions in SSS scores compared to medical care and group exercise, although these did not meet a minimal clinically important difference of 3.02 points. [88] No significant between-group differences were observed in SPWT. Secondary outcomes showed a higher proportion of responders in symptoms and walking capacity with SMT/exercise at two months compared to medical care or group exercise and with no meaningful differences in falls, medical co-interventions, or spinal surgery rates at 6 months.
Neck pain
One RCT studying NP compared the efficacy of three groups: SMT with home exercise, home exercise alone, and supervised exercises plus home exercise. [81] Results favored the SMT plus home exercise group for pain intensity. However, there was no significant between-group difference for disability nor functional status. A higher proportion of participants receiving SMT achieved ≥50% (i.e., substantial) pain reduction at 12 weeks versus controls, although not at 52 weeks or for other thresholds (≥30%, ≥75%). Medication use showed no significant between-group differences. A secondary analysis found SMT plus home exercise reduced total societal costs and improved pain and disability outcomes over 1 year compared to the control intervention. [84] One RCT evaluated the comparative efficacy of SMT treatment duration parameters for NP and disability and found statistically significant differences in favor of long-term management (36 weeks duration) for NP. [82]
Neck and back-related disability
For patients with both neck and back-related disability, one RCT did find statistically significant differences in favor of long-term management (36 weeks duration) for functional status, but there were no significant between-group differences for neck or back-related disability, quality of life, or medication use. [82] Additionally, Maiers et al. (2019) explored responder analysis but did not find any statistically significant differences between groups receiving 12 or 36 weeks of SMT in the proportions reaching 15%, 30%, or 50% improvement in disability.
Reporting biases
A search of ClinicalTrials.gov did not identify any RCTs which were completed yet unpublished. Among included studies, one did not receive funding, [20] and six received funding from non-industry sources [27–29, 81–83]. The lack of industry funding suggests a low likelihood of publication bias. Specific extracted funding sources from included studies can be found in Appendix 5.
Certainty of evidence
The certainty of evidence regarding SMT vs. comparator for LBP was low for pain intensity, back-specific disability status, and functional status. The certainty regarding SMT parameters for LBP was very low for pain intensity and back-specific disability status when comparing thrust vs. non-thrust SMT. The certainty of evidence regarding SMT parameters for LBP was low for pain intensity, back-specific disability status, functional status, and quality of life or activities of daily living (QoL/ADLs) when comparing duration of SMT treatment. The certainty of evidence regarding SMT vs. comparator for LBP was very low for QoL/ADLs. The certainty of evidence regarding SMT for LSS was moderate for back-specific functional status and QoL/ADLs. The certainty of evidence regarding SMT for LSS was very low for pain intensity and was downgraded as no trials were identified that reported this outcome.
The certainty of evidence regarding SMT vs. comparator for NP was low for pain intensity, neck-specific disability status, and functional status. The certainty of evidence regarding SMT parameters for NP was low for pain intensity, neck-specific disability status, functional status, and QoL/ADLs when comparing the duration of SMT treatment. The certainty of evidence regarding SMT vs comparator for NP was very low for QoL/ADLs. All downgrades were due to imprecision, risk of bias, or a lack of identifying studies for the outcome. Appendices 6–10 provide additional detail for graded certainty of evidence for interventions.
Discussion
This systematic review evaluated the efficacy of SMT for chronic spinal conditions in older adults. All results either favored the null or SMT. Significant between-group differences in outcomes favoring SMT over comparators were NP reduction with low certainty of evidence, and significant but small improvements in back-specific functional status in LSS with moderate certainty of evidence. [88, 89] However, there was moderate certainty of evidence favoring the null for QoL in LSS. There was mixed very low and low certainty of evidence for parameters for LBP pain intensity and disability favoring the null. There was very low certainty of evidence for QoL for LBP and NP comparators and LSS pain intensity due to no relevant studies.
Several outcomes demonstrated improvement but were not significantly different compared to active comparators, indicating a lack of additive benefit of SMT over other active interventions (e.g., physical therapy-related interventions such as exercise or physiotherapy) and a lack of superiority in head-to-head comparisons. One study found no significant difference versus an inert comparator. [29] Importantly, there were no outcomes where comparators were superior to SMT. Overall, the certainty of evidence ranged from very low to moderate due to the limited number of trials in this population, imprecision, and risk of bias. A detailed summary of study characteristics can be found in Table 2.
The mixed results identified in the present review may be explained by several factors. First, the focus on chronic condition treatment could lower the likelihood of identifying meaningful changes within and between groups, as the majority of studies were chronic NP and LBP. [90]
Second, most RCTs utilized an active treatment as a comparator. Therefore, null outcomes indicate a lack of additional benefit over these comparators rather than a lack of absolute benefit from SMT, and the efficacy of interventions may be better informed by superiority, noninferiority, and equivalence clinical trial study designs. [91] For example, Enix et al. used a head-to-head design demonstrating similar benefits between SMT and physical therapy. [27]
Finally, some responder analyses demonstrated favorability towards SMT interventions despite initial null outcomes when looking at within group differences for four [28, 81–83] of the included studies as outlined in Appendix 3. This may indicate a trend towards efficacy of SMT or that there are subgroups of patients that respond particularly well to SMT and some that do not. Further research is warranted to clarify these subgroups, as few RCTs of interventions for chronic LBP report responder analyses.92
There were limited data across all conditions, with only four RCTs for LBP and one each for LSS, NP, and neck and back disability analyses. Even for LBP, the most studied condition, the available evidence fell short of ideal standards for synthesis, with fewer than 400 patients per comparison and fewer than five studies. [40, 93] This small amount of RCTs is not unexpected, considering older adults are often excluded from clinical studies. [94] A recent bibliometric analysis95 showed that only one in 10 publications on LBP involved older adults. Future research ought to include this population to better understand LBP prevalence and management approaches. The relatively few studies, coupled with clinical heterogeneity, resulted in very low to moderate certainty per GRADE and hindered definitive conclusions despite some positive findings.
Our findings suggest SMT is a viable treatment option for older adults with chronic LBP, LSS, and chronic NP. While added benefits beyond comparator groups were infrequent in our analyses, there was often a lack of significant differences compared to other standard-of-care comparators like physical therapy or exercise, and there were no unfavorable outcomes for SMT across nine reports of seven RCTs. Non-pharmacological treatments are valued among older adult patients and their clinicians, especially in the context of polypharmacy. [96]
Therefore, clinicians should consider SMT as a treatment option when caring for older adults with chronic LBP, chronic NP, or LSS. There are several factors relevant to SMT and older adults that were beyond the scope of this review and which warrant additional study, such as economic considerations, maintenance of function and quality of life, or patient preferences and satisfaction; there is a need for an update of comprehensive guidelines for the use of SMT in managing chronic spinal conditions in older adults. [97]
Limited evidence for SMT in older adults with chronic LBP, LSS, and chronic NP highlights the need for more high-quality large-sample RCTs dedicated to older adult populations to clarify efficacy, enable meta-analysis, and inform clinical practice guidelines. Accordingly, future RCTs should explore areas of research gaps identified herein including pain, disability, identification of SMT responders versus non-responders, cost-effectiveness, and healthcare utilization. Until more robust data become available, clinicians may rely on this review, observational studies (i.e. case series, case-control studies, longitudinal retrospective or prospective cohort studies incorporating medical records or administrative data, or data from clinical registries), and practice guidelines to guide decision-making.
Strengths and limitations
Strengths of this review include protocol registration, adherence to PRISMA 2020 guidelines, a comprehensive search with librarian input and PRESS review, and duplicate independent screening, extraction, and GRADE assessments.
Our findings had several limitations. First, we deviated from the a priori protocol to include a study that defined chronic LBP as greater than 6 weeks, as opposed to the greater than 12 weeks that we had defined. After consideration, we felt it was appropriate to include Schulz et al. because, at baseline, 96% of their participants reported that their pain episode duration was 12 weeks or longer. Next, we limited our study intervention inclusion to studies that included spinal manipulation as part of the treatment arm. It is unclear if the outcome effects of SMT significantly differ from mobilization, and this limit reduced the number of eligible studies reported.
The small number of RCTs and limited sample sizes per comparison, often drawn from single studies per outcome, led to imprecise effect estimates, and as expected, precluded meta-analysis. Focusing on English-language studies may have introduced selection bias. Many extracted outcomes were stand-alone, reported in only one study, limiting robust synthesis. By prioritizing outcomes from RCTs only, the review overlooked broader healthcare utilization and effectiveness measures like cost, surgery likelihood, or medication use in older adults that may be derived from observational studies. [98–101
Inclusion of observational studies may have afforded better real-world generalizability, yet potentially would introduce risk of bias, and was outside the predetermined scope of our review. While we reported individual item responses from the SIGN checklist and discussed them as a team to provide deeper insights into each study’s reporting, our evidence certainty assessment primarily relied on overall quality ratings derived from thresholds of total scores.
We acknowledge that this approach may oversimplify the risk-of-bias assessment, as certain items may have a disproportionate influence on study outcomes. Future reviews may benefit from using Cochrane tools to assess risk-of-bias at a more granular or domain-based level.
This review did not assess adverse events or safety outcomes, which were beyond the scope of our a priori objectives. Generally, precautions to the use of SMT in older adults include factors that compromise bone density or quality and increase the risk of fracture, such as long-term use of corticosteroids or the presence of osteoporosis. [21, 102] An ideal safety evaluation would require a substantially larger sample size than was available in the seven RCTs included herein, which included 1,226 patients.
Considering the rarity of serious adverse events (i.e., severe [considerable interference], catastrophic [life-threatening, death]) of 1 per 2 million manipulations to 13 per 10,000 patients receiving SMT, [21, 102, 103] large observational studies having several thousand patients (e.g., cohort or case-control designs) are better suited to estimate incidence and characterize risk. A separate systematic review focused on the safety of SMT in older adults is currently in progress, which includes some members of the current author team (PROSPERO CRD42024629286).
Conclusion
There is very low to moderate certainty that SMT may offer comparable or modestly greater efficacy than other treatments for older adults with chronic LBP, chronic NP, and LSS. NP intensity reduction and LSS functional status favored SMT, but other outcomes demonstrated no additive benefit or superiority over comparators, and no comparators were superior to SMT. These comparators included non-thrust manipulation plus a home exercise program, sham treatment, medical care, multimodal physical therapy exercise, treatment duration as well as different combinations of supervised, home-based, and group-based exercise. Certainty was limited due to relatively few trials, imprecision, and risk of bias. There is need for additional high-quality RCTs to clarify the efficacy of SMT for chronic spinal conditions in the older adult population. Overall, SMT is as efficacious as other conservative treatments and can be considered an option for patients and clinicians, provided there are no contraindications to care.
Supplementary Material
To review Appendix 1-10, please refer to the Full Text Omline article.
Acknowledgments
We wish to thank the following individuals whose participation informed and enriched the work: Dennis Enix, DC, MBA, provided additional information and clarifications regarding their team’s study 27, Jennifer Smith, MLIS, AHIP audited our search strategy using the PRESS checklist and providing constructive feedback, and biostatistician Clair Smith, MS assisted with the analysis.
Conflicts of Interest:
The authors wish to disclose that Robert J. Trager, an author on this study, reports earning royalties from authoring texts on the topic of sciatica, and received consulting fees from Merck for participation in an expert input meeting on chronic low back pain (October 2025). The authors have no further disclaimers or competing interest to report in the preparation of this manuscript. Partial funding for this study was received from both Clinical Compass and the NCMIC Foundation
Authors’ contributions
AS and CD contributed to the design, implementation and supervision of the study.
All authors contributed to the study methodology.
SW developed and completed the literature search.
MP and RW performed title, abstract and full-text screening.
RT and JS extracted and interpreted the data and performed risk of bias assessment, and reporting bias was evaluated by CD.
GRADE assessment was performed by AS and CD with assistance from RT and JS.
AS, CD, RT, and JS all participated in drafting the manuscript. All authors read and provided critical review of the manuscript
References:
Global, regional, and national burden of low back pain, 1990–2020, its attributable risk factors, and projections to 2050: a systematic analysis of the Global Burden of Disease Study 2021
Lancet Rheumatol. 2023;5(6):e316–e329GBD 2021 Neck Pain Collaborators.
Global, regional, and national burden of neck pain, 1990–2020, and projections to 2050: a systematic analysis of the Global Burden of Disease Study 2021.
Lancet Rheumatol. 2024;6(3):e142–e155.
doi: 10.1016/S2665-9913(23)00321-1.Rundell SD, Sherman KJ, Heagerty PJ, Mock CN, Jarvik JG.
The Clinical Course of Pain and Function in Older Adults with a New Primary Care Visit for Back Pain.
J Am Geriatr Soc. 2015;63(3):524–530.
doi: 10.1111/jgs.13241.Dionne CE, Dunn KM, Croft PR.
Does back pain prevalence really decrease with increasing age? A systematic review.
Age Ageing. 2006;35(3):229–234.
doi: 10.1093/ageing/afj055.Beliveau PJH, Wong JJ, Sutton DA, et al.
The Chiropractic Profession: A Scoping Review of
Utilization Rates, Reasons for Seeking Care,
Patient Profiles, and Care Provided
Chiropractic & Manual Therapies 2017 (Nov 22); 25: 35Himelfarb I, Johnson CD, Green BN, Bond GD, Shotts BL, Ouzts NE.
Practice Analysis of Chiropractic 2025
National Board of Chiropractic Examiners. Greeley CO: 2025WHO Guideline for Non-Surgical Management of Chronic Primary Low Back Pain in Adults in Primary and Community Care Settings
World Health Organization; 2023Qaseem A, Wilt TJ, McLean RM, et al.
Noninvasive Treatments for Acute, Subacute, and Chronic
Low Back Pain: A Clinical Practice Guideline From
the American College of Physicians
Annals of Internal Medicine 2017 (Apr 4); 166 (7): 514–530Chou R, Qaseem A, Snow V, et al.
Diagnosis and Treatment of Low Back Pain: A Joint Clinical
Practice Guideline from the American College of Physicians
and the American Pain Society
Annals of Internal Medicine 2007 (Oct 2); 147 (7): 478–491Anderson BR, MacKenzie TA, Lurie JD, Grout L, Whedon JM.
Patterns of Initial Treatment and Subsequent Care
Escalation Among Medicare Beneficiaries with
Neck Pain: A Retrospective Cohort Study
European Spine J 2025 (Feb); 34 (2): 724–730Davis M, Yakusheva O, Liu H, Anderson B, Bynum J.
The Effect of Reduced Access to Chiropractic Care
on Medical Service Use for Spine Conditions
Among Older Adults
J Manipulative Physiol Ther 2021 (Jun); 44 (5): 353–362Anderson BR, Whedon JM, Herman PM.
Dosing of lumbar spinal manipulative therapy and its association with escalated spine care: A cohort study of insurance claims
PloS One. 2024 (Jan 5); 19 (1): e0283252Hawk C, Schneider M, Dougherty P, Gleberzon BJ, Killinger LZ.
Best Practices Recommendations for Chiropractic Care
for Older Adults: Results of a Consensus Process
J Manipulative Physiol Ther 2010 (Jul); 33 (6): 464–473Hawk C, Schneider MJ, Haas M, et al.
Best Practices for Chiropractic Care for Older Adults:
A Systematic Review and Consensus Update
J Manipulative Physiol Ther 2017 (May); 40 (4): 217–229Trager RJ, Bejarano G, Perfecto RPT, Blackwood ER, Goertz CM.
Chiropractic and Spinal Manipulation: A Review of Research
Trends, Evidence Gaps, and Guideline Recommendations
J Clin Med. 2024 (Sep 24); 13 (19): 5668Jenks A, de Zoete A, van Tulder M, Rubinstein SM.
Spinal Manipulative Therapy in Older Adults
with Chronic Low Back Pain: An Individual
Participant Data Meta-analysis
European Spine Journal 2022 (Jul); 31 (7): 1821–1845Page MJ, McKenzie JE, Bossuyt PM, et al.
The PRISMA 2020 statement: an updated guideline for reporting systematic reviews.
doi: 10.1136/bmj.n71. Published online March 29, 2021.Older persons.
UNHCR; Jun 13, 2025. [Accessed July 29, 2025]Zulman DM, Sussman JB, Chen X, Cigolle CT, Blaum CS, Hayward RA.
Examining the Evidence: A Systematic Review of the Inclusion and Analysis of Older Adults in Randomized Controlled Trials.
J Gen Intern Med. 2011;26(7):783–790.
doi: 10.1007/s11606-010-1629-x.Learman KE, Showalter C, O’Halloran B, Cook CE.
Thrust and Nonthrust Manipulation for Older Adults With Low Back Pain: An Evaluation of Pain and Disability.
J Manipulative Physiol Ther. 2013;36(5):284–291.
doi: 10.1016/j.jmpt.2013.05.007.Chu ECP, Trager RJ, Lee LYK, Niazi IK.
A Retrospective Analysis of the Incidence of
Severe Adverse Events Among Recipients of
Chiropractic Spinal Manipulative Therapy
Sci Rep 2023 (Jan 23); 13 (1): 1254By the 2019 American Geriatrics Society Beers Criteria® Update Expert Panel.
American Geriatrics Society 2019 Updated AGS Beers Criteria® for Potentially Inappropriate Medication Use in Older Adults.
J Am Geriatr Soc. 2019;67(4):674–694.
doi: 10.1111/jgs.15767.Sfeir JG, Drake MT, Khosla S, Farr JN.
Skeletal Aging.
Mayo Clin Proc. 2022;97(6):1194–1208.
doi: 10.1016/j.mayocp.2022.03.011.McGowan J, Sampson M, Salzwedel DM, Cogo E, Foerster V, Lefebvre C.
PRESS Peer Review of Electronic Search Strategies: 2015 Guideline Statement.
J Clin Epidemiol. 2016;75:40–46.
doi: 10.1016/j.jclinepi.2016.01.021Corporation for Digital Scholarship.
Zotero; Published online 2025
https://www.zotero.org/Ouzzani M, Hammady H, Fedorowicz Z, Elmagarmid A.
Rayyan—a web and mobile app for systematic reviews.
Syst Rev. 2016;5(1):210.
doi: 10.1186/s13643-016-0384-4.Enix D, Malmstrom T, Flaherty J.
A randomized controlled trial of chiropractic compared to physical therapy for chronic low back pain in community dwelling geriatric patients.
2015;6(1):6Schulz C, Evans R, Maiers M, Schulz K, Leininger B, Bronfort G.
Spinal Manipulative Therapy and Exercise for Older Adults
with Chronic Low Back Pain: A Randomized Clinical Trial
Chiropractic & Manual Therapies 2019 (May 15); 27: 21Dougherty PE, Karuza J, Dunn AS, Savino D, Katz P.
Spinal Manipulative Therapy for Chronic Lower Back Pain
in Older Veterans: A Prospective, Randomized,
Placebo-Controlled Trial
Geriatric Orthopaedic Surgery and Rehab. 2014 (Dec); 5 (4): 154–164Satterthwaite FE.
An Approximate Distribution of Estimates of Variance Components.
Biom Bull. 1946;2(6):110–114.
doi: 10.2307/3002019.Chapter 6: Choosing effect measures and computing estimates of effect.
[Accessed March 11, 2025].
https://training.cochrane.org/handbook/current/chapter-06Checklists SIGN.
[Accessed May 13, 2025].
https://testing36.scot.nhs.ukHootman JM, Driban JB, Sitler MR, Harris KP, Cattano NM.
Reliability and validity of three quality rating instruments for systematic reviews of observational studies.
Res Synth Methods. 2011;2(2):110–118.
doi: 10.1002/jrsm.41.Harbour R, Lowe G, Twaddle S.
Scottish Intercollegiate Guidelines Network: the first 15 years (1993–2008)
J R Coll Physicians Edinb. 2011;41(2):163–168.
doi: 10.4997/JRCPE.2011.209.Hawk C, Minkalis AL, Khorsan R, et al.
Systematic Review of Nondrug, Nonsurgical
Treatment of Shoulder Conditions
J Manipulative Physiol Ther 2017 (Jun); 40 (5): 293–319Hawk C, Whalen W, Farabaugh RJ, et al.
Best Practices for Chiropractic Management of
Patients with Chronic Musculoskeletal Pain:
A Clinical Practice Guideline
J Altern Complement Med 2020 (Oct); 26 (10): 884–901Farabaugh R, Hawk C, Taylor D, et al.
Cost of Chiropractic Versus Medical Management of
Adults with Spine-related Musculoskeletal Pain:
A Systematic Review
Chiropractic & Manual Therapies 2024 (Mar 6); 32: 8Weis CA, Stuber K, Murnaghan K, Wynd S.
Adverse Events From Spinal Manipulations in
the Pregnant and Postpartum Periods:
A Systematic Review and Update
J Can Chiropr Assoc 2021 (Apr); 65 (1): 32–49
Enjoy their first (2012) studyArmijo-Olivo S, Fuentes J, da Costa BR, Saltaji H, Ha C, Cummings GG.
Blinding in Physical Therapy Trials and Its Association with Treatment Effects: A Meta-epidemiological Study.
Am J Phys Med Rehabil. 2017;96(1):34–44.
doi: 10.1097/PHM.0000000000000521.Murad MH, Mustafa RA, Schünemann HJ, Sultan S, Santesso N.
Rating the certainty in evidence in the absence of a single estimate of effect.
Evid Based Med. 2017;22(3):85–87.
doi: 10.1136/ebmed-2017-110668.Dwan K, Gamble C, Williamson PR, Kirkham JJ
Reporting Bias Group. Systematic review of the empirical evidence of study publication bias and outcome reporting bias – an updated review.
PloS One. 2013;8(7):e66844.
doi: 10.1371/journal.pone.0066844.Dubin JA, Hameed D, Baksh N, et al.
Impact of Reporting Bias, Conflict of Interest, and Funding Sources on Quality of Orthopaedic Research.
J Arthroplasty. 2024;39(5):1348–1352.
doi: 10.1016/j.arth.2023.11.017..Ziai H, Zhang R, Chan AW, Persaud N.
Search for unpublished data by systematic reviewers: an audit.
BMJ Open. 2017;7(10):e017737.
oi: 10.1136/bmjopen-2017-017737Balshem H, Helfand M, Schünemann HJ, et al.
GRADE guidelines: 3. Rating the quality of evidence.
J Clin Epidemiol. 2011;64(4):401–406.
oi: 10.1016/j.jclinepi.2010.07.015Guyatt GH, Oxman AD, Kunz R, et al.
GRADE guidelines 6. Rating the quality of evidence--imprecision.
J Clin Epidemiol. 2011;64(12):1283–1293.
doi: 10.1016/j.jclinepi.2011.01.012.Guyatt GH, Oxman AD, Kunz R, et al.
GRADE guidelines: 7. Rating the quality of evidence--inconsistency.
J Clin Epidemiol. 2011;64(12):1294–1302.
doi: 10.1016/j.jclinepi.2011.03.017Guyatt GH, Oxman AD, Kunz R, et al.
GRADE guidelines: 8. Rating the quality of evidence--indirectness.
J Clin Epidemiol. 2011;64(12):1303–1310.
doi: 10.1016/j.jclinepi.2011.04.014.Schünemann HJ, Neumann I, Hultcrantz M, et al.
GRADE guidance 35: update on rating imprecision for assessing contextualized certainty of evidence and making decisions.
J Clin Epidemiol. 2022;150:225–242.
doi: 10.1016/j.jclinepi.2022.07.015Weigel PA, Hockenberry J, Bentler SE, Wolinsky FD.
The Comparative Effect of Episodes of Chiropractic and
Medical Treatment on the Health of Older Adults
J Manipulative Physiol Ther 2014 (Mar); 37 (3): 143–154Holt KR, Haavik H, Elley CR.
The Effects of Manual Therapy on Balance and Falls:
A Systematic Review
J Manipulative Physiol Ther. 2012 (Mar); 35 (3): 227–234Weigel PA, Hockenberry J, Bentler S, Wolinsky FD.
Chiropractic Use and Changes in Health Among
Older Medicare Beneficiaries: A Comparative
Effectiveness Observational Study
J Manipulative Physiol Ther 2013 (Nov); 36 (9): 572-584Kendall JC, French SD, Hartvigsen J, Azari MF.
Chiropractic Treatment Including Instrument-assisted Manipulation
for Non-specific Dizziness and Neck Pain in Community-dwelling
Older People: A Feasibility Randomised Sham-controlled Trial
Chiropractic & Manual Therapies 2018 (May 10); 26: 14Maiers M, Evans R, Hartvigsen J, Schulz C, Bronfort G.
Adverse Events Among Seniors Receiving Spinal Manipulation
and Exercise in a Randomized Clinical Trial
Manual Therapy 2015 (Apr); 20 (2): 335–341Maicki T, Bilski J, Szczygie? E, Tr?bka R.
PNF and manual therapy treatment results of patients with cervical spine osteoarthritis.
J Back Musculoskelet Rehabil. 2017;30(5):1095–1101.
doi: 10.3233/BMR-169718.Beselga C, Neto F, Alburquerque-Sendín F, Hall T, Oliveira-Campelo N.
Immediate effects of hip mobilization with movement in patients with hip osteoarthritis: A randomised controlled trial.
Man Ther. 2016;22:80–85.
doi: 10.1016/j.math.2015.10.007Buyukturan O, Buyukturan B, Sas S, Kararti C, Ceylan I.
The effect of Mulligan mobilization technique in older adults with neck pain: a randomized controlled, double-blind study.
Pain Res Manag. 2018 May;:152856375.
doi: 10.1155/2018/2856375. Epub. Published online 2018Kocaman H, Y?ld?z NT, Canl? M, Alkan H.
Comparison of the Effects of Mulligan Mobilization Technique Combined With Cervical Stabilization Exercises With the Effects of Cervical Stabilization Exercises Alone in Chronic Neck Pain: Randomized Controlled Study.
Karya J Health Sci. 2023;4(3):227–234.
doi: 10.52831/kjhs.1374767.Bostan A, Kaya P.
Effect of instrument-assisted soft tissue mobilization combined with exercise therapy on pain and muscle endurance in patients with chronic neck pain: a randomized controlled study.
J Man Manip Ther Taylor Francis Ltd. 2024;32(2):131–140.
doi: 10.1080/10669817.2023.2213989.Domingues L, Pimentel-Santos FM, Cruz EB, et al.
Is a combined programme of manual therapy and exercise more effective than usual care in patients with non-specific chronic neck pain? A randomized controlled trial.
Clin Rehabil. 2019;33(12):1908–1918.
doi: 10.1177/0269215519876675.Gandolfi M, Geroin C, Valč N, et al.
Does myofascial and trigger point treatment reduce pain and analgesic intake in patients undergoing onabotulinumtoxinA injection due to chronic intractable migraine?
Eur J Phys Rehabil Med. 2018;54(1):1–12.
doi: 10.23736/S1973-9087.17.04568-3.Brochado FT, Jesus LH, Carrard VC, Freddo AL, Chaves KD, Martins MD.
Comparative effectiveness of photobiomodulation and manual therapy alone or combined in TMD patients: a randomized clinical trial.
Braz Oral Res. 2018;32:e50.
doi: 10.1590/1807-3107bor-2018.vol32.0050.Farooq MN, Mohseni-Bandpei MA, Gilani SA, Ashfaq M, Mahmood Q.
The effects of neck mobilization in patients with chronic neck pain: A randomized controlled trial.
J Bodyw Mov Ther. 2018;22(1):24–31.
doi: 10.1016/j.jbmt.2017.03.007.Rodríguez-Sanz J, Malo-Urriés M, Corral-de-Toro J, et al.
Does the Addition of Manual Therapy Approach to a Cervical Exercise Program Improve Clinical Outcomes for Patients with Chronic Neck Pain in Short-and Mid-Term? A Randomized Controlled Trial.
Int J Environ Res Public Health. 2020;17(18)
doi: 10.3390/ijerph17186601.Ulger O, Demirel A, Oz M, Tamer S.
The effect of manual therapy and exercise in patients with chronic low back pain: Double blind randomized controlled trial.
J Back Musculoskelet Rehabil. 2017;30(6):1303–1309.
doi: 10.3233/BMR-169673.Avila L, da Silva MD, Neves ML, et al.
Effectiveness of Cognitive Functional Therapy Versus Core Exercises and Manual Therapy in Patients With Chronic Low Back Pain After Spinal Surgery: Randomized Controlled Trial.
Phys Ther. 2024;104(1)
doi: 10.1093/ptj/pzad105Garrigós-Pedrón M, La Touche R, Navarro-Desentre P, Gracia-Naya M, Segura-Ortí E.
Effects of a Physical Therapy Protocol in Patients with Chronic Migraine and Temporomandibular Disorders: A Randomized, Single-Blinded, Clinical Trial.
J Oral Facial Pain Headache. 2018;32(2):137–150.
doi: 10.11607/ofph.1912.Espí-López GV, Rodríguez-Blanco C, Oliva-Pascual-Vaca A, Molina-Martínez F, Falla D.
Do manual therapy techniques have a positive effect on quality of life in people with tension-type headache? A randomized controlled trial.
Eur J Phys Rehabil Med. 2016;52(4):447–456Haller H, Lauche R, Cramer H, et al.
Craniosacral Therapy for the Treatment of Chronic Neck Pain: A Randomized Sham-controlled Trial.
Clin J Pain. 2016;32(5):441–449.
doi: 10.1097/AJP.0000000000000290.Licciardone JC, Gatchel RJ, Aryal S.
Recovery From Chronic Low Back Pain After Osteopathic Manipulative Treatment: A Randomized Controlled Trial.
J Am Osteopath Assoc. 2016;116(3):144–155.
doi: 10.7556/jaoa.2016.031.González-Rueda V, López-de-Celis C, Bueno-Gracia E, et al.
Short-and mid-term effects of adding upper cervical manual therapy to a conventional physical therapy program in patients with chronic mechanical neck pain. Randomized controlled clinical trial
Clin Rehabil”. 2021;35(3):378–389.
doi: 10.1177/0269215520965054.González-Rueda V, Hidalgo-García C, Rodríguez-Sanz J, et al.
Does Upper Cervical Manual Therapy Provide Additional Benefit in Disability and Mobility over a Physiotherapy Primary Care Program for Chronic Cervicalgia? A Randomized Controlled Trial.
Int J Environ Res Public Health. 2020;17(22)
doi: 10.3390/ijerph17228334Pillastrini P, Banchelli F, Guccione A, et al.
Global Postural Reeducation in patients with chronic nonspecific neck pain: cross-over analysis of a randomized controlled trial.
Med Lav. 2018;109(1):16–30.
doi: 10.23749/mdl.v109i1.6677Ariza-Mateos MJ, Cabrera-Martos I, Ortiz-Rubio A.
Effects of a Patient-Centered Graded Exposure Intervention Added to Manual Therapy for Women With Chronic Pelvic Pain: A Randomized Controlled Trial.
Arch Phys Med Rehabil. 2019;100(1):9–16.
doi: 10.1016/j.apmr.2018.08.188.Lehtola V, Luomajoki H, Leinonen V, Gibbons S, Airaksinen O.
Sub-classification based specific movement control exercises are superior to general exercise in sub-acute low back pain when both are combined with manual therapy: A randomized controlled trial.
BMC Musculoskelet Disord. 2016;17:135.
doi: 10.1186/s12891-016-0986-yHanson L, Haas M, Bronfort G, et al.
Dose-response of Spinal Manipulation for
Cervicogenic Headache: Study Protocol
for a Randomized Controlled Trial
Chiropractic & Manual Therapies 2016 (Jun 8); 24: 23Zafereo J, Wang-Price S, Roddey T, Brizzolara K.
Regional manual therapy and motor control exercise for chronic low back pain: a randomized clinical trial.
J Man Manip Ther Taylor Francis Ltd. 2018;26(4):193–202.
doi: 10.1080/10669817.2018.1433283Krekoukias G, Gelalis ID, Xenakis T, Gioftsos G, Dimitriadis Z, Sakellari V.
Spinal mobilization vs conventional physiotherapy in the management of chronic low back pain due to spinal disk degeneration: a randomized controlled trial.
J Man Manip Ther Taylor Francis Ltd. 2017;25(2):66–73.
doi: 10.1080/10669817.2016.1184435.Barker KL, Newman M, Stallard N, et al.
Exercise or manual physiotherapy compared with a single session of physiotherapy for osteoporotic vertebral fracture: three-arm PROVE RCT.
Health Technol Assess Winch Engl. 2019;23(44):1–318.
doi: 10.3310/hta23440.Minetama M, Kawakami M, Teraguchi M, et al.
Supervised physical therapy vs. home exercise for patients with lumbar spinal stenosis: a randomized controlled trial.
Spine J Off J North Am Spine Soc. 2019;19(8):1310–1318.
doi: 10.1016/j.spinee.2019.04.009.Ammendolia C, Côté P, Southerst D, et al.
Comprehensive Nonsurgical Treatment Versus Self-directed Care to Improve Walking Ability in Lumbar Spinal Stenosis: A Randomized Trial.
Arch Phys Med Rehabil. 2018;99(12):2408–2419e2.
doi: 10.1016/j.apmr.2018.05.014Maiers M, Bronfort G, Evans R, et al.
Spinal Manipulative Therapy and Exercise
For Seniors with Chronic Neck Pain
Spine J. 2014 (Sep 1); 14 (9): 1879–1889Maiers M, Hartvigsen J, Evans R, et al.
Short or Long-term Treatment of Spinal Disability
in Older Adults with Manipulation and Exercise
Arthritis Care Res (Hoboken). 2019 (Nov); 71 (11): 1516–1524Schneider MJ, Ammendolia C, Murphy DR, et al.
Comparative Clinical Effectiveness of Nonsurgical Treatment
Methods in Patients With Lumbar Spinal Stenosis:
A Randomized Clinical Trial
JAMA Netw Open 2019 (Jan 4); 2 (1): e186828Leininger B, McDonough C, Evans R, Tosteson T, Tosteson AN, Bronfort G.
Cost-effectiveness of Spinal Manipulative Therapy,
Supervised Exercise, and Home Exercise for
Older Adults with Chronic Neck Pain
Spine J. 2016 (Nov); 16 (11): 1292–1304Maiers M, Forte ML.
Association Between Psychosocial Parameters and Response to Chiropractic Care Among Older Adults With Chronic Low Back Pain: Secondary Analysis of a Randomized Clinical Trial.
J Manipulative Physiol Ther. 2021;44(9):675–682.
doi: 10.1016/j.jmpt.2022.03.001.Furlan AD, Pennick V, Bombardier C, van Tulder M
2009 Updated Method Guidelines for Systematic Reviews in the Cochrane Back Review Group.
Spine. 2009;1929;34(18)
doi: 10.1097/BRS.0b013e3181b1c99f.Dworkin RH, Turk DC, Wyrwich KW, et al.
Interpreting the clinical importance of treatment outcomes in chronic pain clinical trials: IMMPACT recommendations.
J Pain. 2008;9(2):105–121.
doi: 10.1016/j.jpain.2007.09.005.Cleland JA, Whitman JM, Houser JL, Wainner RS, Childs JD.
Psychometric properties of selected tests in patients with lumbar spinal stenosis.
Spine J. 2012;12(10):921–931.
doi: 10.1016/j.spinee.2012.05.004.Carlesso C, Piva SR, Smith C, Ammendolia C, Schneider MJ.
Responsiveness of Outcome Measures in Nonsurgical Patients with Lumbar Spinal Stenosis: A Secondary Analysis From a Randomized Controlled Trial.
Spine. 2021;46(12):788.
doi: 10.1097/BRS.0000000000003920Wallwork SB, Braithwaite FA, O’Keeffe M, et al.
The clinical course of acute, subacute and persistent low back pain: a systematic review and meta-analysis.
CMAJ Can Med Assoc J. 2024;196(2):E29–E46.
doi: 10.1503/cmaj.230542Kishore K, Mahajan R.
Understanding Superiority, Noninferiority, and Equivalence for Clinical Trials.
Indian Dermatol Online J. 2020;11(6):890–894.
doi: 10.4103/idoj.IDOJ_130_20.Henschke N, van Enst A, Froud R, Ostelo WGR.
Responder analyses in randomised controlled trials for chronic low back pain: an overview of currently used methods.
Eur Spine J. 2014;23(4):772–778.
doi: 10.1007/s00586-013-3155-0Jackson D, Turner R.
Power analysis for random-effects meta-analysis.
Res Synth Methods. 2017;8(3):290–302.
doi: 10.1002/jrsm.1240Paeck T, Ferreira ML, Sun C, Lin CWC, Tiedemann A, Maher CG.
Are older adults missing from low back pain clinical trials? A systematic review and meta-analysis.
Arthritis Care Res. 2014;66(8):1220–1226.
doi: 10.1002/acr.22261.Zheng DKY, Kawchuk GN, Bussičres AE, et al.
Trends of Low Back Pain Research in Older and Working-Age Adults from 1993 to 2023: A Bibliometric Analysis.
J Pain Res. 2023;16:3325–3341.
doi: 10.2147/JPR.S425672Ali A, Arif AW, Bhan C, et al.
Managing Chronic Pain in the Elderly: An Overview of the Recent Therapeutic Advancements.
Cureus. 10(9):e3293.
doi: 10.7759/cureus.3293.Briggs AM, Slater H, Hsieh E, et al.
System strengthening to support value-based care and healthy ageing for people with chronic pain.
PAIN. 2019;160(6):1240.
doi: 10.1097/j.pain.0000000000001526Farabaugh R, Hawk C, Taylor D, et al.
Cost of Chiropractic Versus Medical Management of
Adults with Spine-related Musculoskeletal Pain:
A Systematic Review
Chiropractic & Manual Therapies 2024 (Mar 6); 32: 8Trager RJ, Cupler ZA, Srinivasan R, Harper EG, Perez JA.
Association between chiropractic spinal manipulation for sciatica and opioid-related adverse events: A retrospective cohort study.
PloS One. 2025;20(1):e0317663.
doi: 10.1371/journal.pone.0317663Trager RJ, Gliedt JA, Labak CM, Daniels CJ, Dusek JA.
Association Between Spinal Manipulative Therapy and
Lumbar Spine Reoperation After Discectomy:
A Retrospective Cohort Study
BMC Musculoskelet Disord 2024 (Jan 10); 25 (1): 46Anderson BR, McClellan SW.
Three Patterns of Spinal Manipulative Therapy for Back Pain
and Their Association With Imaging Studies, Injection
Procedures, and Surgery: A Cohort Study
of Insurance Claims
J Manipulative Physiol Ther 2021 (Nov); 44 (9): 683–689Swait G, Finch R.
What Are the Risks of Manual Treatment of the Spine?
A Scoping Review for Clinicians
Chiropractic & Manual Therapies 2017 (Dec 7); 25: 37Funabashi M, Gorrell LM, Pohlman KA, Bergna A, Heneghan NR Group on behalf of the A.
Defining and Classifying Adverse Events Following Joint
Manipulation and Mobilization: An International
e-Delphi Study and Focus Groups
PLoS One 2025 (Nov 17); 20 (11): e0334151
Return to LOW BACK PAIN
Return to CHRONIC NECK PAIN
Since 7-04-2026
| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |