

Analysis of State Insurance Coverage for Nonpharmacologic
Treatment of Low Back Pain as Recommended by the
American College of Physicians GuidelinesThis section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: Glob Adv Health Med 2019 (Jul 29); 8: 2164956119855629 ~ FULL TEXT
OPEN ACCESS Robert Bonakdar, MD, Dania Palanker, JD, MPP,
and Megan M Sweeney, MPH
Center on Health Insurance Reforms,
Health Policy Institute at Georgetown University,
Washington, District of Columbia.
FROM: Weeks ~ JMPT 2016 (Feb) Hurwitz ~ JMPT 2016 (May)Background: In 2017, the American College of Physicians (ACP) released guidelines encouraging nonpharmacologic treatment of chronic low back pain (LBP). These guidelines recommended utilization of treatments including multidisciplinary rehabilitation, acupuncture, mindfulness-based stress reduction (MBSR), tai chi, yoga, progressive relaxation, biofeedback, cognitive behavioral therapy (CBT), and spinal manipulation.
Objective: We aimed to determine status of insurance coverage status for multiple nonpharmacological pain therapies based on the 2017 Essential Health Benefits (EHB) benchmark plans across all states.
Methods: The 2017 EHB benchmark plans represent the minimum benefits required in all new policies in the individual and small group health insurance markets and were reviewed for coverage of treatments for LBP recommended by the ACP guidelines. Additionally, plans were reviewed for limitations and exclusionary criteria.
Results: In nearly all state-based coverage policies, chronic pain management and multidisciplinary rehabilitation were not addressed. Coverage was most extensive (supported by 46 states) for spinal manipulation. Acupuncture, massage, and biofeedback were each covered by fewer than 10 states, while MBSR, tai chi, and yoga were not covered by any states. Behavioral health treatment (CBT and biofeedback) coverage was often covered solely for mental health diagnoses, although excluded for treating LBP.
Conclusion: Other than spinal manipulation, evidence-based, nonpharmacological therapies recommended by the 2017 ACP guidelines were routinely excluded from EHB benchmark plans. Insurance coverage discourages multidisciplinary rehabilitation for chronic pain management by providing ambiguous guidelines, restricting ongoing treatments, and excluding behavioral or complementary therapy despite a cohesive evidence base. Better EHB plan coverage of nondrug therapies may be a strategy to mitigate the opioid crisis. Recommendations that reflect current research-based findings are provided to update chronic pain policy statements.
Keywords: chronic pain; complementary and alternative medicine; health policy; integrative medicine; public health.
From the FULL TEXT Article:
Background
Low back pain (LBP) is the leading cause of years lost to disability worldwide, and in the United States, the leading cause of disability for Americans under 45 years of age. [1, 2] Individuals not only face extreme adversity in daily functioning; LBP also imposes a significant financial burden on the American economy—estimated at $100 billion—primarily attributable to lost wages and limited productivity. [3, 4] The incidence of LBP and price of subsequent care have been rapidly increasing, calling into question the efficacy and cost-effectiveness of current treatment approaches. [5] A prominent aspect is the overreliance, prolonged use, and subsequent abuse of opioids. A recent cross-sectional study of adults with chronic LBP in the United States found that opioids were the most commonly administered prescription pain medication. [6] The use of opioid was considered long term in 75% of individuals with LBP, and prescriptions were frequently coadministered with antidepressants, benzodiazepines, and hypnotics. [7] Although treatment of LBP is highly determined by payor coverage, opioid administration may also be influenced by socioeconomic status. [8] Prior research has suggested that individuals of a lower socioeconomic status were 63% more likely to receive opioid therapy, as opposed to multiple nonpharmacological options that were more frequently offered to people of higher socioeconomic statuses. [9–11]
Recent evidence has challenged common therapies for LBP. Treating chronic LBP with opioids augments the risk of adverse outcomes, and these pharmacologic strategies have not been proven a more effective or superior to nonopioid therapies. [12, 13] As increasing evidence supports the clinical benefits, cost-efficacy, and safety of nonpharmacological therapies, these safer alternatives are increasingly incorporated into formal protocols for chronic pain treatments. Recommendations for nonpharmacological treatment considerations of chronic pain are now supported by the U.S. Center for Disease Control, [14] Institute of Medicine, [15] The National Pain Strategy, [16] the Veterans Health Administration and Department of Defense, [17] and the Academic Consortium for Integrative Medicine and Health. [18]
One of the most anticipated guidelines specific to the treatment of LBP was published in 2017 by the American College of Physicians (ACP). [19] The 2017 recommendations aimed to encompass available evidence for nonpharmacological approaches to pain management—including multidisciplinary rehabilitation, exercise, acupuncture, mindfulness-based stress reduction (MBSR), tai chi, yoga, progressive relaxation, biofeedback, cognitive behavioral therapy (CBT), and spinal manipulation. The recommendations also heavily emphasized the use of select nonpharmacologic treatments for the initial management of chronic LBP.
Despite multiple recommendations encouraging clinicians to initially prioritize use of nonpharmacologic treatments for the management of LBP, gaps remain between evidence-based guidelines and standard clinical practices. [20] One of the primary factors driving this inconsistency has been attributed to payment models, which may restrict coverage for nonpharmacologic therapies. The shortfalls associated with lack of coverage may impose the greatest burden on individuals with the utmost need for coverage of nonpharmacological therapies such as those who rely primarily on the Essential Health Benefits (EHB).
The EHB are the basic set of insurance benefits that most health plans sold in the individual and small group markets within each of the 50 states and the District of Columbia must cover. The EHB were created through the Affordable Care Act and require health plans in the individual and small group markets to cover 10 broad categories of health benefits [21]: ambulatory patient services; emergency services; hospitalization; maternity and newborn care; mental health and substance use disorder services, including behavioral health treatment; prescription drugs; rehabilitative services and devices; laboratory services; preventive and wellness services and chronic disease management; and pediatric services, including oral and vision care. [22] Defining each of the 10 EHB categories was left to the U.S. Department of Health and Human Services, which created a process for each state and the District of Columbia to choose from one of the 10 existing plans for sale in the state and to create a benchmark plan by supplementing any categories or otherwise specified requirements that were not covered by the chosen plan. [23] For example, there was a process for states to add maternity coverage, habilitative services, and pediatric dental and vision to the EHB benchmarks if they were not in the state’s chosen plan. Although coverage policies are a key element in utilizing health services, an information gap exists surrounding coverage of nonpharmacologic therapies for chronic LBP that constrains policy development and implementation processes.
Each states’ benefits are detailed in the certificates of coverage that are provided to enrollees in the benchmark insurance plan. Aspects provided in the benchmark plans vary by state and coverage category. The benchmark plans do not detail specific diagnoses or procedures that are covered within each category. [21] Individual and small group market health insurance plans must provide the services in the EHB benchmarks as a minimum. Replacements and substitutions must also be explained (eg, a plan may replace chiropractic care with acupuncture) if the visit limits are the same. While plans may provide additional benefits, significant variation is limited in the individual market because the premium subsidies that reduce the cost of insurance to enrollees only apply to the EHB packages. Although nonpharmacological strategies for managing pain have demonstrated effectiveness, the availability, affordability, and accessibility to such treatments are often limited by overarching policies. [24] The present study aimed to review the 2017 state-by-state EHB benchmarks to assess the landscape of coverage pertaining to nonpharmacological treatments of chronic LBP. We did not pursue formal hypothesis testing or infer causal pathways surrounding official coverage policies.
Methods
The 2017 EHB benchmark plan coverage manuals and summary statements for each state and the District of Columbia published by the Centers for Medicare & Medicaid Services were electronically identified. [21] Authors reviewed plan information for treatments recommended by the ACP guidelines including acupuncture, biofeedback, CBT, yoga, MBSR, tai chi, progressive relaxation, massage, and manipulation. We aimed to determine coverage for multidisciplinary rehabilitation as a well as massage, tai chi, and yoga as distinct entities beyond traditionally covered physical therapies.
Each EHB benchmarks for all 50 states and the District of Columbia were reviewed for coverage determination. Nonpharmacological treatments were coded via binomial classification according to coverage status. Unmentioned, unclear, or contradictory treatments were coded as “not covered.” This classification is supported by policy statements shown to exclude services not specifically mentioned by default. [25]
Additionally, plans were reviewed to determine whether:
Mental health treatments, including CBT, were exclusively covered for disorders classified in the Diagnostic and Statistical Manual of Mental Disorders, 5th Edition (DSM-5®) [26] implying lack of coverage for pain conditions (DSM-5 exclusions).
Complementary and alternative medicine (CAM) therapies were excluded based on plan designations (CAM exclusion). This incorporated exclusion based on wording such as complementary, alternative, holistic, or nontraditional.
Massage was covered as a distinct entity as opposed to a subcomponent of physical and manipulative therapy that may not be billed by certain providers (eg, massage therapists).
Chronic pain or pain management in the nonacute, nonpalliative setting was mentioned as a distinct entity.
Multidisciplinary rehabilitation was mentioned and whether it was described as a distinct multiprofession collaborative therapy.
Tai chi, yoga, and MBSR were designated “not covered.” In cases where individual or group exercise, fitness, recreation, or stress management therapies were not covered, exclusions were noted.
Other exclusions and limitations were listed for the above therapies including practitioner exclusions, visit limits, and requirements for combined therapies. The process for coverage determinations was consistent within policy statements.
Results
Analysis of Nonpharmacological Treatments
Manipulation Manipulation, chiropractic, or osteopathic coverage determination was noted in plan information for all states. Coverage was recorded in a binary fashion regardless of the type of professional providing the treatment. Spinal manipulation was covered in 46 states and the District of Columbia. Four states (California, Colorado, Hawaii, and Oregon) did not cover manipulation. In several benchmarks, manipulation was only covered for acute musculoskeletal disorders and not a benefit when provided for chronic conditions. In most other benchmarks, there was not clear elaboration of coverage for chronic conditions.

Table 1 Acupuncture Acupuncture coverage determination was noted in plan information for all states. Five states (Arkansas, California, Maryland, New Mexico, and Washington) consider acupuncture an EHB. In 1 additional state (Montana), acupuncture was noted as a benefit in the summary statement, despite contradiction in the official coverage manual under CAM exclusions. [27] Based on the discrepancy, acupuncture was categorized as not covered, therefore confirming coverage in 5 total states. See Table 1 for details.
Massage Massage or massage therapy coverage determinations were identified in 37 states’ plans. Of these, 28 plans did not cover massage either explicitly (13 states) or cited it within a CAM exclusion (15 states). Two states (West Virginia and Maine) regarded massage a covered treatment but simultaneously listed it as a CAM exclusion. Three states (Illinois, Texas, and Florida) appeared to cover massage but either did not have specifics on coverage or excluded certain types of massage. Four states only covered massage if administered by physical therapists (California and New Mexico), chiropractors (Louisiana), or both practitioners (Minnesota). Given the restrictions on which health professionals were approved to administer massage, the subsequent 4 states were not included in the cohesive coverage count in states supporting massage therapy. Detailed plan information deemed massage could not be billed as a separate entity or by other licensed therapists such as massage therapists. Based on these subtle restrictions, the levels of coverage for massage as a distinct entity performed by a massage therapist are likely less than noted.
Biofeedback Biofeedback coverage determination was evident in 30 states’ plans. Biofeedback was specifically mentioned as a covered benefit for pain management in 1 state (Arizona) plan. The remaining 29 state policies explicitly deny biofeedback for various reasons, including unconditional denial of biofeedback, denial based on biofeedback based on CAM designation, or denial based on coverage of biofeedback for medical conditions that did not include LBP. The most commonly cited, covered medical conditions were incontinence, Raynaud’s disease, and headache disorders. Of note, 1 state (Florida) plan excluded biofeedback in 1 section (as a CAM exclusion) but cited it as a covered benefit in an additional area. Another (Michigan) mentioned biofeedback as potentially covered based on medical necessity “as determined according to our medical policies.” Based on the general level of denial in other state plans, this was deemed as unclear and categorized as not covered.
Cognitive behavioral therapy Specific CBT coverage determinations were noted in 2 states’ plans with pain coverage remaining unclear. In 1 state (Connecticut), CBT was noted as a covered benefit, although the plan stated, “There is no coverage for other conditions not defined as mental disorders in the most recent edition of the American Psychiatric Association’s DSM-5®,” although CBT may be covered under behavioral services when not specifically noted, the DSM-5® was noted in 39 other plans and was frequently leveraged in denial of coverage for behavioral services for conditions including chronic pain.
Multidisciplinary rehabilitation and chronic pain management We attempted to determine the likelihood of multidisciplinary rehabilitation and chronic pain management in EHB plans. Nearly, all plans failed to specifically address chronic pain. In 1 state (Iowa) plan, there were only 3 mentions of “pain” — all of which pertained to treatment of acute or emergent pain. When chronic pain was mentioned in 1 state (Alabama) plan, it was in the context of denying treatment: “The following services and supplies are not covered: … Treatment for chronic pain … .” [28] Similarly, multidisciplinary rehabilitation defined as “multidimensional rehabilitation” composed of a minimum of the physical dimension and one of the other related dimensions (psychological, social, or occupational) as a distinct entity beyond unimodal physical therapy was not mentioned and could not be evaluated in several coverage statements. [29] A potential exception in 1 plan (Florida) noted, “Pain Management includes, but is not limited to, services for pain assessment, medication, physical therapy, biofeedback, and/or counseling. Pain rehabilitation programs are programs featuring multidisciplinary services directed toward helping those with chronic pain to reduce or limit their pain.” This plan also excluded nonpharmacological treatments (eg, biofeedback), thereby contradicting coverage for multidisciplinary rehabilitation.
Specific exercise programs and stress management programs (yoga, tai chi, MBSR) State policies were analyzed for coverage of practitioner and modality-specific exercise and stress management programs distinct from traditional physical therapy. These programs were discussed minimally in coverage statements. Yoga was mentioned in 5 state policies (Florida, Georgia, Michigan, New York, and Rhode Island) and was noted as a noncovered benefit due to exclusion of CAM therapies or exercise in all states. Tai chi was only mentioned in 1 plan (Rhode Island) and deemed not covered. MBSR was not included within any policy statements. Other types of stress management programs (eg, meditation) were noted in 10 states — 7 of which deemed meditation not covered due to CAM exclusions. Three states provided some type of stress management typically in an online or phone-based coaching. Finally, a small number of states mentioned potential discounts at fitness centers, although coverage specifics and availability of treatments was unclear.
Nonspecific exclusions Even if nonpharmacological therapies were originally noted as covered options for patients diagnosed with LBP, plan information for all states incorporated several exclusions and limitations that influenced ultimate coverage status of important treatments noted in the ACP guidelines. Specific exclusionary criteria are reviewed in Table 1.
While at least 7 states did not limit number of annual treatments, most states capped number of visits for single modalities, which were as low as 10 treatments per year (eg, manipulation). A number of states placed combination treatment limits (as low as 20) for 2 or more modalities. In 1 state (Washington), a total of 20 combined yearly treatments were available for manipulation, physical, and occupational therapy.
Although most plan information did not specifically mention the process for determining coverage, some states did elaborate on potential sources of coverage. One example noted that claims were based, among other factors, on review of sources including, “Generally accepted standards of medical, behavioral health and dental practice based on credible scientific evidence recognized in published peer reviewed medical or dental literature.” [30]
CAM exclusions In addition to the exclusion of behavioral treatments for pain as noted above, a number of the ACP recommended treatments were also excluded due to their designation in state plans as CAM therapies. At least 27 states had wording which excluded treatments that were deemed complementary, alternative, holistic or nontraditional. No standard listing of treatments was noted, although acupuncture, biofeedback, massage, and biofeedback were often listed. In some cases (eg, biofeedback in Florida), treatments were both listed as covered under the policy statement as well as not covered under CAM exclusions. The rationale used for denial of services was typically not explained.
Behavioral health for pain exclusions While mental and behavioral treatments are listed as EHB, explicit coverage for such therapies for pain management was rare. A number of states as noted above had wording excluding behavioral health treatments provided for nonmental health diagnosis such as pain. The rational utilized was that only treatment listed in the DSM would be covered (DSM exclusions). [26]
Specific practitioner/therapist exclusions Qualifications of practitioners mandated to administer nonpharmacological treatments (eg, manipulation and massage) added further ambiguity in state-by-state determination of coverage. Plans typically characterized coverage of manipulation under “chiropractic services” in summary statements, while a number of states incorporated a distinct section on osteopathic manual medicine — manipulation therapy performed by a doctor of osteopathy. The opposite was true for massage, which proved to be covered only when administered by a physical therapist or chiropractor, while massage provided by a massage therapist was often denied.
Discussion
The EHB provision to the Affordable Care Act intended to provide individual and small group market insurance participants health coverage in fundamentally important areas. This was partially enacted based on prior evidence that increased coverage may potentially improve chronic disease care and subsequent health outcomes. [31] While health coverage has demonstrated positive effects on management of chronic conditions such as depression, there has been little evaluation of this potential in the setting of chronic pain. [32] An essential first step to address this gap in the evidence was to evaluate coverage for evidence-based chronic pain treatments.
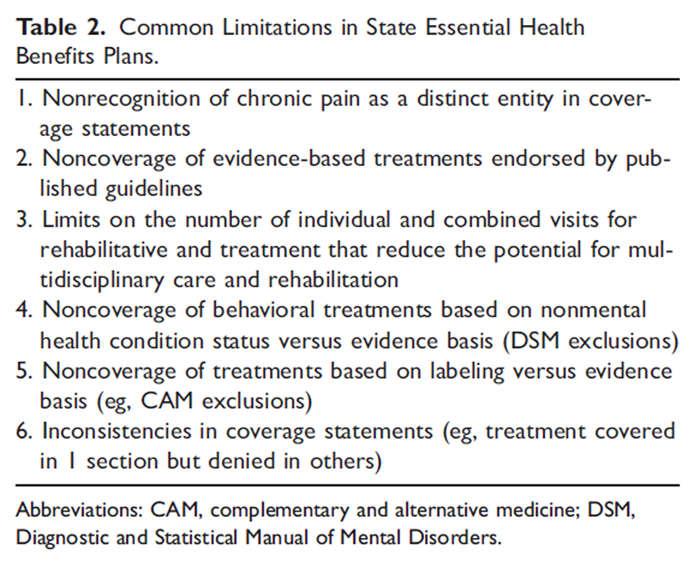
Table 2 The ACP recommendations for the treatment of chronic LBP are likely the most prominent and influential guidelines in this area. Analysis of 2017 EHB benchmarks for level of coverage for ACP-recommended treatments in all 50 states and the District of Columbia distinguished several flaws. First, except for manipulation, the evidence-based treatments recommended by the ACP guidelines are included in fewer than 10 states’ benchmark plans. In cases where coverage was identified, caps were often placed on the number of treatments, which may limit treatments to adequately address chronic pain. Several recommended treatments — namely, multidisciplinary rehabilitation, biofeedback, and CBT — were difficult to evaluate due to inconsistent or unclear policy statements. Finally, coverage limitations associated with chronic conditions further reduce therapeutic opportunities. Table 2 details the aforementioned limitations in policy statements.
Chronic pain is one of the most burdensome and expensive conditions plaguing the United States. While many stakeholders have identified incorporation of nonpharmacological treatment as a potential solution, the overall level of denial and ambiguity related to coverage is concerning. [14] Additionally, minimal recognition of chronic pain as a distinct entity within policy statements illuminates a lack of awareness surrounding the condition as well as deficits in policy support for appropriate treatments. As noted in the 2018 National Pain Strategy, coverage arrangements can “… exert powerful effects on how pain is managed and may lead pain patients to gravitate to prescription drugs over complementary or alternative treatments, creating risks for subsequent problems with opioid dependency.” [15]
Evidence-based treatments consistently change with new technology and influence the “medically necessary” classifications at a given point in time. Accordingly, a mechanism to periodically review translational research, clinical guidelines, and treatments in terms of medical necessity is warranted. Since delays in therapies and overreliance on unimodal interventions have shown to increase treatment costs and risks, it is imperative that policy statements clearly address chronic pain and multidisciplinary treatments to reduce this burden. [33] In addition, socioeconomically disadvantaged individuals have demonstrated greater reliance on EHB coverage for chronic disease care because premiums are subsidized for eligible low-income participants in the insurance marketplaces. [34] Rural and underserved communities appear to have much higher rates of opioid prescriptions, opioid-related hospitalizations, and drug overdose deaths, which may stem, in part, from the lack of nonpharmacological treatment coverage. [35] Finally, the noncoverage of treatments based on labeling (CAM exclusion) that is outdated and largely inconsistent between states appears arbitrary and potentially discriminatory.
Clinical and research institutions must be strengthened to enable systematic evaluation of evidence in the context of policy constraints and facilitate focused interactions between researchers and policymakers. The present study validates findings reported by previous investigations of EHB provisions and reinforces how overarching policies hinder clinical practices. A recent review of commercial and Medicare insurers found that while coverage was available for manipulation and physical therapies, the majority of plans denied or lacked information on acupuncture and psychological interventions despite supporting evidence. [36]
Notably, expansion of coverage for these therapies may have immediate clinical and financial benefit. Several states that do not support coverage for nonpharmacological treatments have attempted expansion of evidence-based services. For example, a state-funded trial expanded acupuncture coverage for chronic pain in Vermont’s Medicaid population. This pragmatic trial found that in addition to improved pain status, patients receiving acupuncture for chronic pain, 57% and 32% were able to reduce nonopioid and opioid analgesics, respectively, and an additional 91% reported qualitative improvements in physical, functional/behavioral, or psycho-emotional status. [37] Preceding research has also revealed that initial treatments with yoga, acupuncture, manipulation, MBSR, and CBT, in the setting of LBP are cost-effective. [38, 39]
States have recently had the option to amend their EHB offerings to reflect new evidence-based research findings. Some states (eg, Montana) have clarified prior discrepancies in their policies to reflect positive changes in coverage. Illinois remains the only state that has chosen to update the 2018 policy statement, which mandates coverage in 2020. The amendments to the Illinois policy emphasize the importance of mental health treatments, exercise and physical reconditioning, nutrition, as well as complementary and alternative modalities as first-line interventions for pain management. [22]
Despite the notable findings, limitations of this review cannot be dismissed. The EHB present a floor and some insurance plans provide additional benefits or replace some of the EHB services with other covered benefits. Discussions with plan administrators to clarify areas of coverage (eg, coverage status in the individual and small group markets despite denial in the EHB) were not included. Coverage could also be overestimated in states that deny treatments according to specific chronic condition criteria.
Table 3 We chose to focus on treatment modalities that are often initiated and maintained by certified modality specific practitioners which may have underestimated coverage. For example, massage, tai chi, yoga, and MSBR were noncovered when they were explicitly listed due to specific noncoverage statements or practitioner and CAM-related exclusions. Because physical therapy is universally covered, many of these specific therapies may be covered based on the training of the physical therapist. However, the frequency and extent of incorporation as a component of physical therapy visit could not be presently determined. Similarly, several states cited discounts at fitness centers that could theoretically cover exercise therapies recommended in ACP guidelines. Because the type and level of coverage and availability could not be ascertained, they were noted as excluded and may have also underestimated coverage. Table 3 provides recommendations for clarifying EHB benchmark plans and increasing treatment access.
Conclusion
Analysis of the 2017 EHB benchmark plans that represent the minimum benefits required in all states demonstrated that, other than manipulation, there was significant lack of coverage for nonpharmacological treatments recommended by the ACP guidelines for chronic LBP. Although state EHB coverage policies should reflect current evidence, our analysis reveals a disconnect between evidence-based recommendations and official guidelines. Statements often used outdated, arbitrary, and contradictory language to justify denial of treatments, a practice that appears to be largely unchanged since 2017 when EHB modifications were permitted. For individuals who depend on EHB coverage as a strong determinant of chronic pain management, it is especially vital for states to ensure access to comprehensive options including nonpharmacological treatments to improve the current trajectory of pain care in America.
In anticipation of future revisions to EHB benchmark plans, states should increasingly aim to enact policies that reflect safe, evidence-based, and efficacious treatment options in effort to address the alarming rates of chronic pain as well as substantial societal costs. Recommendations are provided for revising policy statements to better reflect current evidence and suggestions for treating chronic pain.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References:
Vos T, Allen C, Arora M, et al.
Global, Regional, and National Incidence, Prevalence, and Years Lived
with Disability for 310 Diseases and Injuries, 1990-2015: a Systematic
Analysis for the Global Burden of Disease Study 2015
Lancet. 2016 (Oct 8); 388 (10053): 1545–1602National Centers for Health Statistics.
Chartbook on Trends in the Health of Americans.
http://www.cdc.gov/nchs/data/hus/hus06.pdf.
Published 2006. Accessed May 25, 2019.Gaskin DJ, Richard P.
The economic costs of pain in the United States.
J Pain. 2012; 13(8):715–724Katz JN.
Lumbar disc disorders and low-back pain:
socioeconomic factors and consequences.
J Bone Joint Surg Am. 2006; 88(2):21–24Deyo RA, VonKorff M, Duhrkoop D.
Opioids for low back pain.
BMJ. 2015; 350:g6380Waljee JF, Brummett CM.
Opioid prescribing for low back pain: what is the role of payers?
JAMA Netw Open. 2018; 1(2):e180236Shmagel A, Ngo L, Ensrud K, Foley R.
Prescription medication use among community-based U.S. adults with
chronic low back pain: a cross-sectional population-based study.
J Pain. 2018; 19(10):1104–1112Lin DH, Jones CM, Compton WM, et al.
Prescription drug coverage for treatment of low back pain
among us Medicaid, Medicare Advantage, and commercial insurers.
JAMA Network Open. 2018; 1(2):e180235Becker WC, Dorflinger L, Edmond SN, Islam L, Heapy AA, Fraenkel L.
Barriers and facilitators to use of
non-pharmacological treatments in chronic pain.
BMC Fam Pract. 2017; 18(1):41Gebauer S, Salas J, Scherrer JF.
Neighborhood socioeconomic status and receipt of
opioid medication for new back pain diagnosis.
J Am Board Fam Med. 2017; 30(6):775–783Chuang E, Gil EN, Gao Q, Kligler B, McKee MD.
Relationship between opioid analgesic prescription and unemployment
in patients seeking acupuncture for chronic pain in urban primary care.
Pain Med. doi:10.1093/pm/pny169Fields HL.
The doctor’s dilemma: opiate analgesics and chronic pain.
Neuron. 2011; 69(4):591–594Krebs EE, Gravely A, Nugent S, et al.
Effect of opioid vs nonopioid medications on pain-related function
in patients with chronic back pain or hip or knee osteoarthritis pain:
the SPACE randomized clinical trial.
JAMA. 2018; 319(9):872–882Dowell D, Haegerich TM, Chou R.
CDC guideline for prescribing opioids for chronic pain—United States, 2016.
JAMA. 2016; 315(15):1624–1645Institute of Medicine (IOM)
Relieving Pain in America: A Blueprint for Transforming
Prevention, Care, Education, and Research
Washington, DC: The National Academies Press, 2011.Interagency Pain Research Coordinating Committee.
National Pain Strategy: A Comprehensive Population
Health-Level Strategy for Pain
Washington, DC: US Department of Health and Human Services,
National Institutes of Health; 2016.Kerns RD, Philip EJ, Lee AW, Rosenberger PH.
Implementation of the veterans health administration national pain management strategy.
Transl Behav Med. 2011; 1(4):635–643H. Tick, A. Nielsen, K.R. Pelletier, R. Bonakdar, S. Simmons, R. Glick
Evidence-Based Nonpharmacologic Strategies for Comprehensive Pain Care:
The Consortium Pain Task Force White Paper
Explore (NY). 2018 (May); 14 (3) 177-211Qaseem A, Wilt TJ, McLean RM, Forciea MA;
Noninvasive Treatments for Acute, Subacute, and Chronic Low Back Pain:
A Clinical Practice Guideline From the American College of Physicians
Annals of Internal Medicine 2017 (Apr 4); 166 (7): 514–530Foster NE, Anema JR, Cherkin D, Chou R, Cohen SP, et al.
Prevention and Treatment of Low Back Pain:
Evidence, Challenges, and Promising Directions
Lancet. 2018 (Jun 9); 391 (10137): 2368–2383
This is the third of 4 articles in the remarkable Lancet Series on Low Back PainCenters for Medicare & Medicaid Services.
Information on Essential Health Benefits (EHB) Benchmark Plans.
https://www.cms.gov/cciio/resources/data-resources/ehb.html#ehb
Accessed November 15, 2018.Essential Health Benefits Requirements, 42 USC §18022.
Giovannelli J, Lucia KW, Corlette S.
Implementing the Affordable Care Act:
revisiting the ACA’s essential health benefits requirements.
Issue Brief (Commonw Fund). 2014; 28:1–10Corlette S, Lucia KW, Levin M.
Implementing the Affordable Care Act:
choosing an essential health benefits benchmark plan.
Issue Brief (Commonw Fund). 2013; 15:1–14Centers for Medicare & Medicaid Services, CCIIO.
Illinois EHB Benchmark Plan
https://www.cms.gov/CCIIO/Resources/Data-Resources/Downloads/
Updated-Illinois-Benchmark-Summary.pdf
Accessed December 29, 2018.American Psychiatric Association.
Diagnostic and Statistical Manual of Mental Disorders (DSM-5®)
Washington, DC: American Psychiatric Publications; 2013.Robert Wood Johnson Foundation.
Essential Health Benefits: 50-state Variations on a Theme
Philadelphia, PA: Leonard Davis Institute of Health Economics,
University of Pennsylvania; 2014.Centers for Medicare & Medicaid Services, CCIIO.
Alabama EHB Benchmark Plan
https://www.cms.gov/CCIIO/Resources/Data-Resources/Downloads/
Updated-Alabama-Benchmark-Summary.pdf
Accessed December 29, 2018.Kamper SJ, Apeldoorn AT, Chiarotto A, et al.
Multidisciplinary biopsychosocial rehabilitation for chronic low back pain:
Cochrane database system review and meta-analysis.
BMJ. 2015; 350(1):h444Centers for Medicare & Medicaid Services, CCIIO.
Georgia EHB Benchmark Plan
https://www.cms.gov/CCIIO/Resources/Data-Resources/Downloads/
Updated-Georgia-Benchmark-Summary.pdf
Accessed December 29, 2018.Furman J.
Six Economic Benefits of the Affordable Care Act
https://obamawhitehouse.archives.gov/blog/2014/02/06/six-economic-
benefits-affordable-care-act
Published 2014. Accessed May 25, 2019.Sommers BD, Gawande AA, Baicker K.
Health insurance coverage and health—what the recent evidence tells us.
N Engl J Med. 2017; 377(6):586–593Reneman MF, Waterschoot FPC, Bennen E, Schiphorst Preuper HR.
Dosage of pain rehabilitation programs:
a qualitative study from patient and professionals’ perspectives.
BMC Musculoskelet Disord. 2018; 19(1):206Palanker D, Volk J, Giovannelli J.
Eliminating Essential Health Benefits Will Shift Financial Risk Back to Consumers.
The Commonwealth Fund. March 24, 2017.
http://www.commonwealthfund.org/publications/blog/2017/mar/eliminating-
essential-health-benefits-financial-risk-consumers.Dasgupta N, Beletsky L, Ciccarone D.
Opioid crisis: no easy fix to its social and economic determinants.
Am J Public Health. 2018; 108(2):182–186Heyward J, Jones CM, Compton WM, et al.
Coverage of Nonpharmacologic Treatments for Low Back Pain
Among US Public and Private Insurers
JAMA Network Open 2018 (Oct 5); 1 (6): e183044Davis R, Badger G, Valentine K, Cavert A, Coeytaux RR.
Acupuncture for chronic pain in the Vermont Medicaid population:
a prospective, pragmatic intervention trial.
Glob Adv Health Med. 2018; 7:2164956118769447Herman PM, Anderson ML, Sherman KJ, Balderson BH, Turner JA, Cherkin DC.
Cost-effectiveness of mindfulness-based stress reduction versus cognitive
behavioral therapy or usual care among adults
with chronic low back pain.
Spine. 2017; 42(20):1511–1520Andronis L, Kinghorn P, Qiao S, Whitehurst DG, Durrell S, McLeod H.
Cost-Effectiveness of Non-Invasive and Non-Pharmacological Interventions
for Low Back Pain: A Systematic Literature Review
Applied Health Econ and Health Policy 2017 (Apr); 15 (2): 73–201Situ D, Wang J, Shao W, Zhu ZH.
Assessment and treatment of cancer pain:
from western to eastern.
Ann Palliat Med. 2012; 1(1):32–44.
Return NON-PHARMACOLOGIC THERAPY
Since 1-19-2023
| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |