

A Commentary on the Use of Mixed Methods
in Chiropractic Research. Part 3:
Integration of Qualitative Research
with Randomized Controlled TrialsThis section was compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: J Can Chiropr Assoc 2024 (Apr); 68 (1): 26-34 ~ FULL TEXT
OPEN ACCESS Peter C. Emary, DC, PhD • Kent J. Stuber, DC, PhD
Michael G. DeGroote Institute for Pain Research and Care,
McMaster University,
Hamilton, Ontario
This is the third of three papers in our series of articles on the use of mixed methods in chiropractic research. In this commentary, we discuss the mixed methods experimental (or intervention) design. This design is a complex mixed methods research design in which qualitative research is integrated with randomized controlled trials.
We provide a brief overview of this study design as well as a case example from the literature to illustrate how this approach can be applied to research within the chiropractic profession.
Keywords: Chiropractic; Mixed Methods; Qualitative Research; Randomized Controlled Trial.
From the FULL TEXT Article:
Introduction
Qualitative research methods can be used alongside randomized controlled trials (RCTs) to help develop and evaluate complex health interventions. [1–3] Chiropractic care, as delivered in ‘real-world’ clinical practice, can be defined as a complex health intervention. For instance, according to Drabble and O’Cathain [2], a complex health intervention is neither a drug or surgical procedure, but rather an intervention that has many active components. These components combine independently and interdependently, “making the whole of the intervention more than the sum of its parts.” [2] Furthermore, complex health interventions can be socially mediated, in that they can take different forms, such as when the behaviours of people delivering or receiving an intervention are variable. [2]
In line with the above definition, chiropractic care typically includes a combination of therapies (e.g., spinal manipulation, soft-tissue therapy, exercises, education, and reassurance) [4], and it often deals with both the physical and biopsychosocial aspects of a patient’s clinical presentation. Within the therapies delivered by a chiropractor, there can also be a myriad of manipulation techniques that might be used in treating the patient, such as Diversified, Gonstead, Cox, Thompson, or Activator Methods, to name a few. Other contextual factors, such as the skill level and experience of the treating practitioner, as well as their ability to communicate and develop a rapport with the patient (i.e., their ‘bed-side manner’), can further influence the doctor-patient encounter and impact the success of the intervention. [5, 6] Such contextual factors are difficult to measure and control for in a controlled research environment. Researchers have also had difficulty establishing an appropriate control intervention (e.g., ‘sham’ manipulation) in RCTs of chiropractic treatment, as the effects of ‘therapeutic touch’ and doctor-patient interaction within the clinical setting can attenuate differences between groups and result in statistically similar outcomes between control and active therapies. [7] Not surprisingly, published RCTs and systematic reviews of RCTs of chiropractic interventions have often had mixed or inconclusive results. [8–13] This is in contrast to numerous observational and qualitative chiropractic research studies that consistently report large associations or positive treatment outcomes and high patient satisfaction. [14–19]
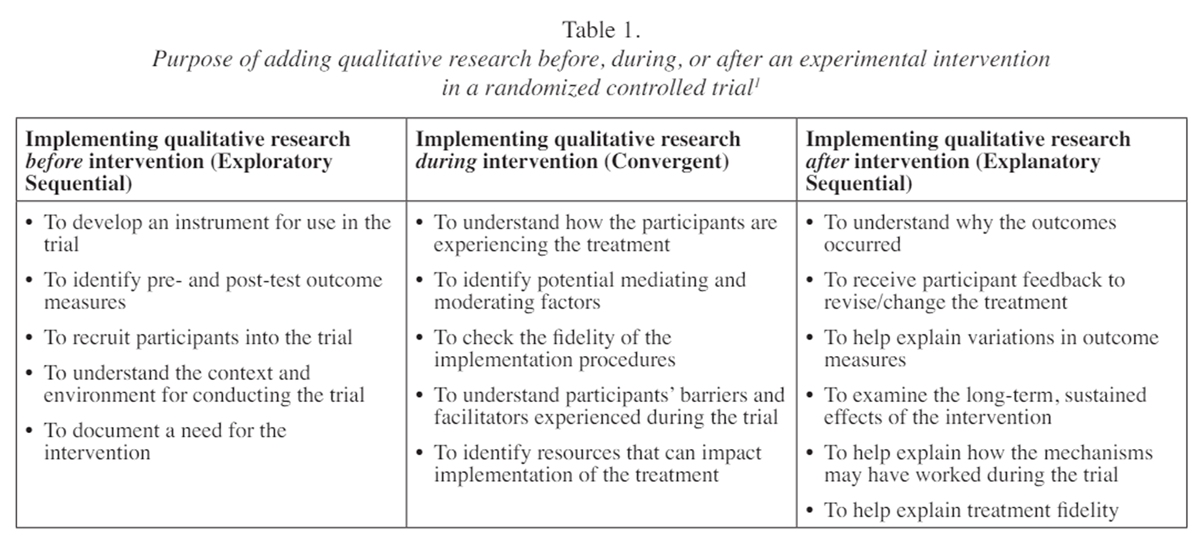
Investigating the efficacy of services provided by chiropractors can be challenging within the context of the traditional (i.e., double-blind, placebo-controlled) RCT. As such, RCTs of chiropractic services could potentially benefit from the addition of qualitative research methods. In particular, these methods would add value within the clinical trial setting in terms of evaluating the design, delivery, and outcomes of chiropractic services, which, as described above, constitute a “complex” therapeutic intervention. For example, qualitative data collected prior to a clinical trial can be used to develop study instruments or inform recruitment procedures. Qualitative data collected during a clinical trial can help investigators understand how participants experience the intervention. When investigators collect qualitative data after a clinical trial, this information can help explain why an intervention may or may not have worked. [1] However, RCTs incorporating qualitative research for such purposes within the chiropractic literature are scarce. [5, 20–23] Outside of the chiropractic profession, the use of qualitative research alongside, or integrated with, RCTs of interventions is also lacking. For example, a 2009 study [3] found that less than one-third of 100 systematically sampled trials registered in the Cochrane Effective Practice and Organization of Care Review Group had associated qualitative work. In 67% of the trials that did, there was no integration of the qualitative and quantitative findings, and the methodological quality of the qualitative studies in these trials was highly variable. [3]
Objective
The purpose of this commentary is to:.(1) review the main reasons for integrating qualitative research within the RCT design, and
(2) highlight how this approach could benefit the chiropractic profession, and its patients,
if utilized more frequently in the design and reporting of chiropractic RCT investigations
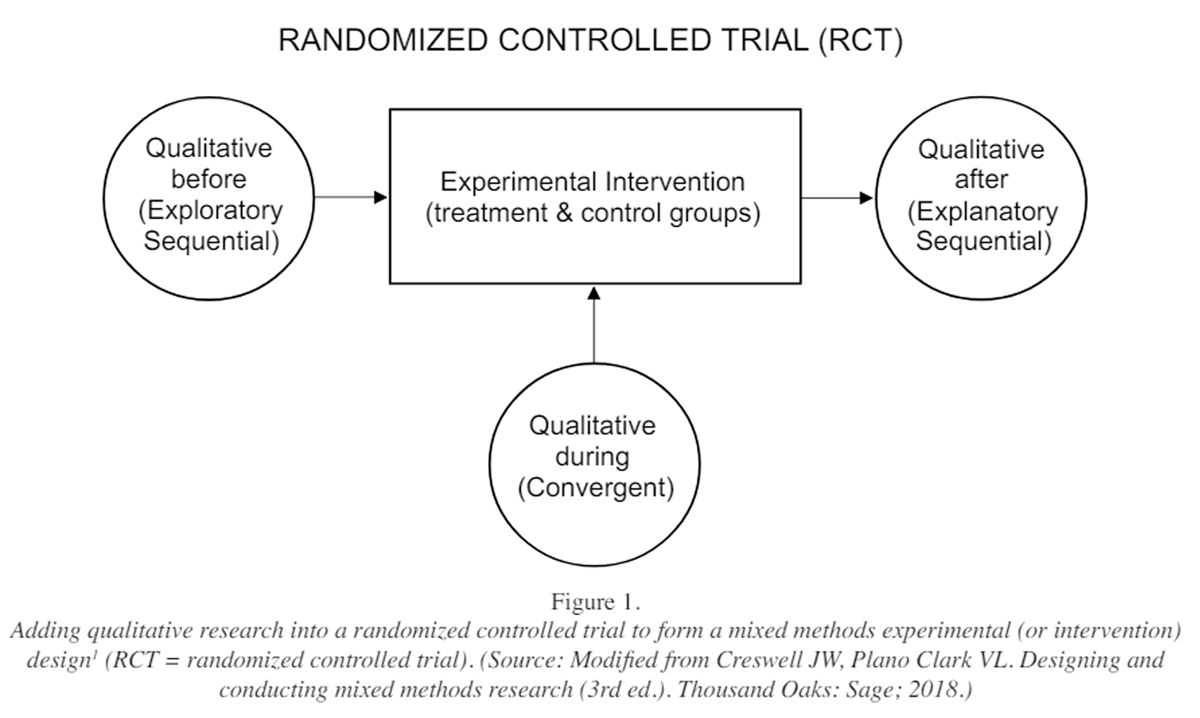
Figure 1 For instance, embedding qualitative methods within chiropractic RCTs can potentially improve the quality of evidence generated from these studies and result in greater understanding of treatment mechanisms or effects for optimizing delivery of care in the clinical setting. This approach is particularly beneficial in RCTs where interventions are provided and delivered at multiple sites and/or by multiple practitioners. We will use a 2016 mixed methods study by Maiers et al. [5] as a case example, and frame our discussion within the mixed methods experimental (or intervention) design, as described by Creswell and Plano Clark [1] (Figure 1). Although our focus in this commentary will be on how integrating qualitative research with RCTs can improve the design and evaluation of such studies in chiropractic, this topic can also be applied to disciplines outside the chiropractic profession.
Discussion
Integration of qualitative research with RCTs:
the mixed methods experimental (or intervention) design
The mixed methods experimental (or intervention) design is used when both quantitative and qualitative data are collected and analyzed, and then integrated, within an experiment or intervention trial such as an RCT. [1] In this design, qualitative data are added as a secondary component to the primary quantitative RCT design to enrich the quantitative results. A core mixed methods design (i.e., exploratory sequential, convergent, or explanatory sequential design a ) is embedded into the RCT either before, during, or after the RCT (see Figure 1).
Integration in the mixed methods experimental design occurs when the results from the qualitative phase of the study connect to or merge with the experimental trial procedures or results. [1] For example, connecting to the trial means integration may occur early in the study and the qualitative findings help shape the planning of the trial procedures1 . When integration occurs during the study (i.e., by ‘merging’ [1] ), qualitative research can be conducted simultaneously with the experimental procedures and used as a separate procedure to examine participants’ experience with the trial process. Alternatively, the integration may occur after the study concludes as a follow-up to help explain the trial outcomes. Investigators may also conduct and integrate qualitative research at multiple points in the trial. Regardless of approach, investigators will draw integrated conclusions (or ‘meta- [1, 24]) at the end of the study based on the combined results.
Benefits and challenges of integrating qualitative research with RCTs

Table 1 The integration of qualitative research with RCTs has the potential to improve the design and conduct of a trial, particularly in pilot studies where researchers are interested in testing the feasibility of the trial’s planning, process, and outcomes. Successful feasibility studies then allow subsequent trials (e.g., Phase III and IV trials) to evaluate the optimum intervention(s), recruit participants efficiently, and measure the right outcomes in a valid way. [1, 2] Integrating qualitative research with RCTs also helps with understanding the process of a clinical trial (e.g., intervention implementation, blinding, fidelity, receipt of co-interventions, etc.), as well as explaining outcomes between intervention and control groups. [1, 2] The understanding of contextual factors or other confounders that may be related to treatment outcomes is particularly relevant in multi-site trials where the ‘same’ treatment may be implemented by providers and received by patients at the different sites in different ways. Integrating qualitative research with RCTs also promotes teamwork among quantitative, qualitative, and mixed methods researchers, and is an appealing mixed methods approach to funding agencies, especially those less familiar with mixed methods research. [1, 2] As described earlier, integrating qualitative research with RCTs is particularly useful when evaluating process or outcomes in clinical trials involving complex therapeutic interventions, such as multi-modal chiropractic care. Common reasons for adding a qualitative study before, during, or after an RCT are listed in Table 1.
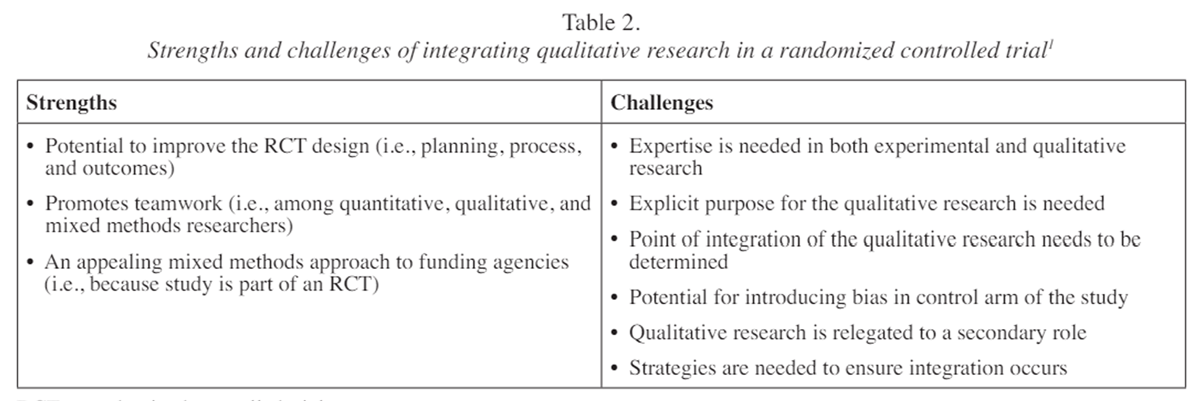
Table 2 There are challenges in integrating qualitative research with RCTs that require careful consideration before implementing this design. [5] For instance, investigators and their research teams need to have sufficient resources and the necessary expertise to conduct both the clinical trial as well as the qualitative research. Investigators need to specify the purpose for collecting qualitative data as part of the larger RCT (e.g., to shape the intervention, explain the process of participants during treatment, or follow up on results of the larger RCT), and determine the appropriate point in the trial to collect qualitative data (i.e., before, during or after the intervention, or at multiple points during the RCT). Investigators also need to ensure that qualitative data collection does not introduce bias into the trial and affect outcomes. Strategies to mitigate this risk include collecting unobtrusive qualitative data to minimize contact between the investigator and participants (e.g., use of patient diaries rather than individual or focus group interviews), equally distributing the qualitative data collection across treatment and control groups, or postponing the qualitative data collection until after the intervention has been completed by using an explanatory sequential approach. [1] In addition, the research team should implement rigorous qualitative methods, highlight the importance of the qualitative research in the study, and ensure that integration strategies such as data transformation, narrative discussion, and/or joint displays1 are employed. A summary of the strengths and challenges of integrating qualitative research with RCTs is provided in Table 2.
Case example from the chiropractic literature Study protocol (Westrom et al. [25])
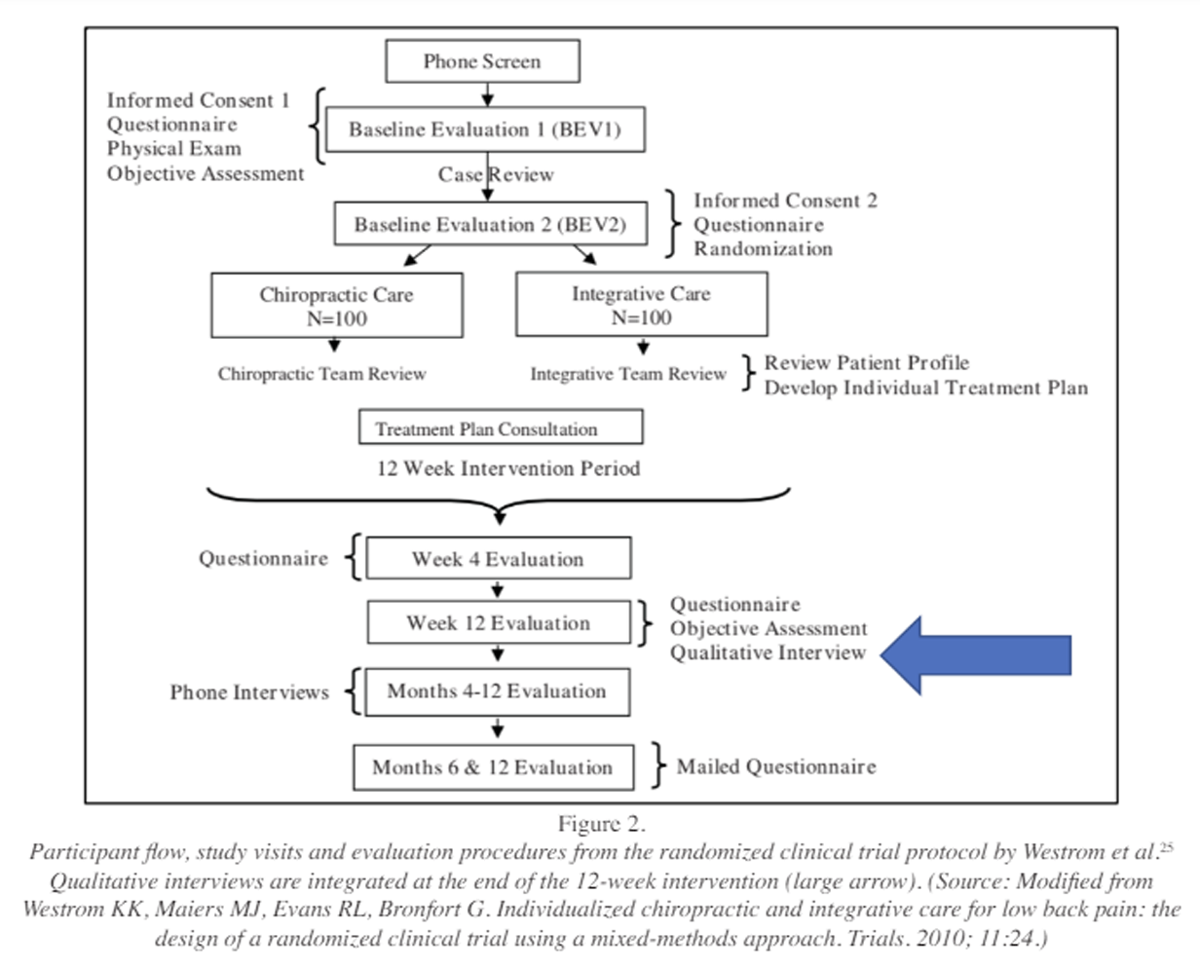
Figure 2 This was a 2010 study protocol for an RCT of 200 adults with non-acute low back pain that compared chiropractic care with multidisciplinary integrative care (i.e., chiropractic, massage, traditional Chinese medicine, psychology, allopathic medicine, and exercise therapy) using a mixed methods experimental design. In this protocol, the authors included team members with expertise in both experimental and qualitive research methods, and the purpose of the qualitative component in the study was to better understand how patients’ experiences and preferences influenced treatment outcomes. [25] To reduce bias, the investigators introduced qualitative research after the 12–week intervention (Figure 2). The qualitative methods for this protocol included semi-structured oneon-one interviews of patients at the end of the 12–week treatment period and with providers at the end of the trial. This study protocol is an example of an explanatory sequential mixed methods design embedded into an RCT after the experimental intervention is complete (see Figure 1).
In a subsequent multi-site study (see ‘Study methods’ below), the authors compared chiropractic care, consisting of high-velocity, low-amplitude spinal manipulative therapy (delivered to the lumbar vertebral or sacroiliac joints) plus home exercise and advice, versus only home exercise and advice in adults with subacute and chronic back-related leg pain [5, 26], using the Westrom et al. [25] mixed methods experimental design protocol. The spinal manipulative therapy was delivered by 11 chiropractors in the study, and was complemented by soft-tissue techniques (e.g., muscle stretching, trigger point therapy, hot and cold packs), while 13 providers, including seven chiropractors, five exercise therapists, and one personal trainer, delivered the home exercise and advice interventions. These interventions consisted of four, one-hour one-onone visits in which patients were given instruction and practice on stabilization exercises (i.e., pelvic tilt, quadruped, bridging, abdominal curl-ups, and side bridging), as well as methods for spine posture awareness related to their activities of daily living, such as lifting, pushing and pulling, sitting, and getting out of bed. [26] Information about simple pain-management techniques, including cold, heat, and movement, as well as printed take-home materials with instructions and photos of the exercises, were also provided.
Study methods
In the protocol by Westrom et al. [25], which was implemented in the studies by Bronfort et al [26] and Maiers et al. [5], patients were asked during 15–minute, in-person interviews how they felt about the treatment they received, whether it met their expectations, and what they liked and disliked about treatment. Patients were also asked to identify factors considered when determining their satisfaction with care. Interviews with providers explored the clinicians’ experiences working with other providers in their respective mono- and multi-disciplinary clinical care teams, as well as the perceived usefulness of the care pathways. An interdisciplinary research team, consisting of three chiropractors and a nurse, all with advanced qualitative research training, conducted content analysis using qualitative data analysis software (NVivo®) to identify and summarize themes.
Study results (Maiers et al. [5])
In the follow-up publication by Maiers et al. [5] , they reported their qualitative findings on participants from within the larger trial. [26] A total of 174 (91%) of 192 participants from the trial completed interviews. Integration was achieved by merging the quantitative and qualitative results through data transformation (i.e., quantifying qualitative data) and through narrative discussion. Notably, participants placed high value on their interactions with study providers (i.e., chiropractors and exercise therapists) and research staff when determining their satisfaction with care (n = 120). This theme was most common among those receiving spinal manipulation plus home exercise and advice, and the authors suggested that this might explain the advantages observed in this group in terms of satisfaction, pain, and disability compared to controls from the parent trial (Bronfort et al. [26]). For instance, in the parent trial by Bronfort et al. [26], spinal manipulation plus home exercise and advice had a clinically important advantage over home exercise and advice for leg pain symptoms (difference, 10 percentage points [95% CI, 2 to 19]) at 12 weeks, with greater global improvement, satisfaction, and reduced medication use also measured in the spinal manipulation plus exercise and advice group at 12 weeks, with sustained improvements at 52 weeks, when compared to participants in the control group. In their interviews, participants in both groups of the study also described changes in other outcomes (i.e., in addition to their back pain and disability), such as with body awareness, emotional well-being, and perceptions of their health and health care, which were not captured in the quantitative self-reported outcomes of the main trial. [5, 26]
Participant quotes from the Maiers et al. [5] study
Among many participants (n = 68) in the spinal manipulation plus home exercise and advice group, patient-provider interactions were viewed favourably and were reflective of the perceived competence, personal attributes, and approach of the chiropractic providers:“ It’s more a personal emotional thing, than a physical thing, it was again that [provider] was so extremely attending to me. He was always, really trying to see the person in me, and work with that, and seek out things. This was what I enjoyed most that I was taken so seriously …”
Sometimes, though, participants expressed concerns about having received treatment from different chiropractic providers during the study:
“ I felt that maybe some days that because it wasn’t the same individual every time, that, the quality was different. Not that it was any worse, it was just different.”
Study implications
The aforementioned quotes from the Maiers et al. [5] study highlight some of the contextual factors (and ‘complexities’) involved in the delivery of chiropractic care, especially when it is delivered in multiple settings and by multiple providers. The authors of this study concluded that the qualitative results provided insight into the quantitative outcomes of the parent clinical trial, particularly around patient-provider relationships and the effect these can have on patient compliance to the interventions and satisfaction with care. In addition, participant-reported changes in health domains outside of spinal pain and disability revealed in the trial may have implications for the use and selection of outcome measures in subsequent trials. These insights gleaned from this study were findings that would not have been obtainable using only the quantitative methods of the larger RCT.
Other examples from the chiropractic literature
In two 2014 mixed methods RCTs on the effect of chiropractic care in chronic neck pain patients, [21, 22] qualitative findings from semi-structured interviews of participants allowed for better interpretation of quantitative outcomes in the parent clinical trials [27, 28] and identified facets of the clinical encounter that contributed to a positive therapeutic experience. [22] In the study by Evans et al. [21], the authors also gained a deeper understanding of the patient-reported outcome measure, Global Perceived Effect, from the perspective of neck pain sufferers and that contextual aspects of treatment (e.g., frequency, dose, and supervision) play an important role in patients’ views of their recovery. Similar to Maiers et al. [5] , both studies minimized additional bias by collecting qualitative data equally between the intervention and control groups, and this was conducted after the intervention was completed. [21, 22] Hence, as illustrated by these and other studies, [5, 20, 23] investigators should consider employing the mixed methods experimental (or intervention) design more frequently in clinical trial research within the chiropractic profession.
We are aware of only two groups, at Northwestern Health Sciences University in Bloomington, Minnesota, USA and Palmer Chiropractic College in Davenport, Iowa, USA that have used the mixed methods experimental (intervention) approach. [5, 20–23] In affiliation with McMaster University in Hamilton, Ontario, Canada, PCE will also be employing a convergent, mixed methods experimental design in a feasibility study on the effect of chiropractic care on opioid use for adults with chronic non-cancer spinal pain. [29] The purpose of incorporating qualitative methods in this study is to understand participants’ experiences within the context of the clinical trial and with the trial process (i.e., recruitment, retention, intervention implementation, and data collection), and this information will be used to inform the design of a larger, definitive cluster RCT.
Conclusion
Despite the challenges of integrating qualitative methods into a quantitative RCT design, this integration can provide for greater insights into the trial’s planning, contextual environment, conduct (or processes), and outcomes.
Because chiropractic care is a complex clinical intervention, where the “whole of the intervention is greater than the sum of its parts,” we feel that qualitative investigation should be prioritized by chiropractic researchers and embedded within their quantitative RCT designs. Doing so will enhance the understanding of these clinical trial outcomes as well as patient and provider experiences, outcome measurement tools, confounding variables, and other contextual factors that may have important implications for future research and clinical practice within the chiropractic profession and other health-related fields.
Acknowledgment
This paper is based on a presentation initially developed by PCE for a graduate-level course on Mixed Methods Research Designs for Health Services and Policy Research in the Department of Health Research Methods, Evidence, and Impact at McMaster University.
References:
Creswell JW, Plano Clark VL.
Designing and conducting mixed methods research (3rd ed.).
Thousand Oaks: Sage; 2018.Drabble SJ, O’Cathain A.
Moving from randomized controlled trials to mixed methods intervention evaluations (Part 3).
In Hesse-Biber SN & Johnson RB (Eds).
The Oxford handbook of multimethod and mixed methods research inquiry.
Oxford Handbooks Online: Oxford University Press; 2018.Lewin S, Glenton C, Oxman AD.
Use of qualitative methods alongside randomised controlled trials of
complex healthcare interventions: methodological study.
BMJ. 2009; 339:b3496.Beliveau PJH, Wong JJ, Sutton DA, Simon NB, Bussičres AE, Mior SA, French SD.
The Chiropractic Profession: A Scoping Review of Utilization Rates,
Reasons for Seeking Care, Patient Profiles, and Care Provided
Chiropractic & Manual Therapies 2017 (Nov 22); 25: 35Maiers M, Hondras MA, Salsbury SA, Bronfort G, Evans R.
What Do Patients Value About Spinal Manipulation and Home Exercise
for Back-related Leg Pain? A Qualitative Study
Within a Controlled Clinical Trial
Manual Therapy 2016 (Dec); 26: 183–191Marthick-Hone D, Doyle AK, Kennedy GA, Vindigni D, Polus BI.
The importance of setting and therapeutic relationships when delivering
chiropractic care to those living with disadvantage.
Chiropr Man Therap. 2022;30(1):47.Puhl AA, Reinhart CJ, Doan JB, Vernon H.
The Quality of Placebos used in Randomized, Controlled Trials of Lumbar
and Pelvic Joint Thrust Manipulation - A Systematic Review
Spine J. 2017 (Mar); 17 (3): 445–456Murphy AYMT, van Teijlingen ER, Gobbi MO.
Inconsistent grading of evidence across countries:
a review of low back pain guidelines.
J Manipulative Physiol Ther. 2006; 29(7):576-581.e2.Rubinstein SM, Terwee CB, Assendelft WJ, de Boer MR, van Tulder MW.
Spinal manipulative therapy for acute low-back pain.
Cochrane Database Syst Rev. 2012; 2012(9):CD008880.Coulter ID, Crawford C, Vernon H, et al.
Manipulation and Mobilization for Treating Chronic Nonspecific Neck Pain:
A Systematic Review and Meta-Analysis for an Appropriateness Panel
Pain Physician. 2019 (Mar); 22 (2): E55–E70Rist PM, Hernandez A, Bernstein C, Kowalski M, Osypiuk K,
Vining R, Long CR, Goertz C, Song R, Wayne PM.
The Impact of Spinal Manipulation on Migraine Pain and
Disability: A Systematic Review and Meta-Analysis
Headache: J Head and Face Pain. 2019 (Apr); 59 (4): 532–542Côté P, Hartvigsen J, Axén I, et al.
The global summit on the efficacy and effectiveness of spinal manipulative therapy
for the prevention and treatment of nonmusculoskeletal disorders:
a systematic review of the literature.
Chiropr Man Therap. 2021;29(1):8.
Erratum in: Chiropr Man Therap. 2021;29(1):11.Asquini G, Pitance L, Michelotti A, Falla D.
Effectiveness of manual therapy applied to craniomandibular structures
in temporomandibular disorders: A systematic review.
J Oral Rehabil. 2022;49(4):442-455.Houweling TA, Braga AV, Hausheer T, Vogelsang M, Peterson C, Humphreys BK.
First-Contact Care With a Medical vs Chiropractic Provider After Consultation
With a Swiss Telemedicine Provider: Comparison of Outcomes,
Patient Satisfaction, and Health Care Costs in Spinal,
Hip, and Shoulder Pain Patients
J Manipulative Physiol Ther. 2015 (Sep); 38 (7): 477–483Weeks WB, Leininger B, Whedon JM, Lurie JD, Tosteson TD, Swenson R, O’Malley AJ, Goertz CM.
The Association Between Use of Chiropractic Care and Costs of Care Among
Older Medicare Patients With Chronic Low Back Pain and Multiple Comorbidities
J Manipulative Physiol Ther. 2016 (Feb); 39 (2): 63–75iller JE, Hanson HA, Hiew M, Lo Tiap Kwong DS, Mok Z, Tee YH.
Maternal Report of Outcomes of Chiropractic Care for Infants
J Manipulative Physiol Ther. 2019 (Mar; 42 (3): 167–176Corcoran KL, Bastian LA, Gunderson CG, Steffens C, Brackett A, Lisi AJ.
Association Between Chiropractic Use and Opioid Receipt Among Patients
with Spinal Pain: A Systematic Review and Meta-analysis
Pain Medicine 2020 (Feb 1); 21 (2): e139–e145Green BN, Johnson CD, Daniels CJ, Napuli JG, Gliedt JA, Paris DJ.
Integration of Chiropractic Services in Military and Veteran Health
Care Facilities: A Systematic Review of the Literature
J Evid Based Complementary Altern Med. 2016 (Apr); 21 (2): 115–130Gaumer G.
Factors Associated With Patient Satisfaction With Chiropractic Care:
Survey and Review of the Literature
J Manipulative Physiol Ther. 2006; 29(6):455-462.Evans RL, Maiers MJ, Bronfort G.
What Do Patients Think? Results of a Mixed Methods Pilot Study Assessing
Sciatica Patients' Interpretations of Satisfaction and Improvement
J Manipulative Physiol Ther. 2003 (Oct); 26 (8): 502–509Evans R, Bronfort G, Maiers M, Schulz C, Hartvigsen J.
"I Know It's Changed": A Mixed-methods Study of the Meaning of
Global Perceived Effect in Chronic Neck Pain Patients
European Spine Journal 2014 (Apr); 23 (4): 888–897Maiers M, Vihstadt C, Hanson L, Evans R.
Perceived Value of Spinal Manipulative Therapy and Exercise Among
Seniors With Chronic Neck Pain: A Mixed Methods Study
J Rehabil Med. 2014 (Nov); 46 (10): 1022–1028Salsbury SA, Goertz CM, Vining RD, et al.
Interdisciplinary Practice Models for Older Adults
With Back Pain: A Qualitative Evaluation
Gerontologist. 2018 (Mar 19); 58 (2): 376–387Fetters MD, Freshwater D.
The 1 + 1 = 3 integration challenge.
J Mix Methods Res. 2015;9(2):115-117.Westrom KK, Maiers MJ, Evans RL, Bronfort G.
Individualized Chiropractic and Integrative Care for Low Back Pain:
The Design of a Randomized Clinical Trial Using a Mixed-methods Approach
Trials 2010 (Mar 8); 11: 24Bronfort G, Hondras MA, Schulz CA, Evans RL, Long CR, Grimm R.
Spinal Manipulation and Home Exercise With Advice for Subacute and
Chronic Back-related Leg Pain: A Trial With Adaptive Allocation
Annals of Internal Medicine 2014 (Sep 16); 161 (6): 381—391Evans R, Bronfort G, Schulz C, Maiers M, Bracha Y, Svendsen K, Grimm R, Garvey T, Transfeldt E.
Supervised Exercise With And Without Spinal Manipulation Performs
Similarly And Better Than Home Exercise For Chronic Neck Pain:
A Randomized Controlled Trial
Spine (Phila Pa 1976). 2012 (May 15); 37 (11): 903–914Maiers M, Bronfort G, Evans R, Hartvigsen J, Svendsen K, Bracha Y, Schulz C, Schulz K, Grimm R.
Spinal Manipulative Therapy and Exercise
For Seniors with Chronic Neck Pain
Spine J. 2014 (Sep 1); 14 (9): 1879–1889Emary PC.
The effect of chiropractic care on opioid use for
chronic spinal pain: a feasibility study.
ClinicalTrials. gov ID: NCT06160947 (Accessed December 18, 2023)
Return to CHIROPRACTIC RESEARCH
Since 6-09-2024
| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |