

Definition and Classification for Adverse Events
Following Spinal and Peripheral Joint
Manipulation and Mobilization:
A Scoping ReviewThis section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: PLoS One 2022 (Jul 15); 17 (7): e0270671 ~ FULL TEXT
OPEN ACCESS Martha Funabashi, Lindsay M Gorrell, Katherine A Pohlman, Andrea Bergna, Nicola R Heneghan
Division of Research and Innovation,
Canadian Memorial Chiropractic College,
Toronto, ON, Canada.
Introduction: Spinal and peripheral joint manipulation and mobilization are interventions used by many healthcare providers to manage musculoskeletal conditions. Although there are many reports of adverse events (or undesirable outcomes) following such interventions, there is no common definition for an adverse event or clarity on any severity classification. This impedes advances of patient safety initiatives and practice. This scoping review mapped the evidence of adverse event definitions and classification systems following spinal and peripheral joint manipulation and mobilization for musculoskeletal conditions in adults.
Methods: An electronic search of the following databases was performed from inception to February 2021: MEDLINE, EMBASE, CINAHL, Scopus, AMED, ICL, PEDro, Cochrane Library, Open Grey and Open Theses and Dissertations. Studies including adults (18 to 65 years old) with a musculoskeletal condition receiving spinal or peripheral joint manipulation or mobilization and providing an adverse event definition and/or classification were included. All study designs of peer-reviewed publications were considered. Data from included studies were charted using a standardized data extraction form and synthesised using narrative analysis.
Results: From 8,48 identified studies, 98 were included in the final synthesis. A direct definition for an adverse event and/or classification system was provided in 69 studies, while 29 provided an indirect definition and/or classification system. The most common descriptors to define an adverse event were causality, symptom severity, onset and duration. Twenty-three studies that provided a classification system described only the end anchors (e.g., mild/minor and/or serious) of the classification while 26 described multiple categories (e.g., moderate, severe).
Conclusion: A vast array of terms, definition and classification systems were identified. There is no one common definition or classification for adverse events following spinal and peripheral joint manipulation and mobilization. Findings support the urgent need for consensus on the terms, definition and classification system for adverse events related to these interventions.
From the FULL TEXT Article:
Introduction
Spinal pain, including low back and neck pain, is the most common musculoskeletal problem globally, a leading cause of disability and absenteeism from work and is ever increasing. [1] These factors contribute to increased socioeconomic burdens and costs. [2] Clinical guidelines and best practice recommendations (e.g., NICE Guidelines) advocate the use of conservative interventions, including spinal and peripheral joint manipulation and mobilization, provided by a variety of healthcare professionals (e.g., chiropractors, naprapaths, osteopaths, physiotherapists, physicians, etc.) as a management option for uncomplicated presentations of spinal pain. [3–5] Used globally by manual therapists as conservative interventions, spinal and peripheral joint manipulation involves the application of a high-velocity, low-amplitude force to a specific joint, whilst spinal and peripheral joint mobilization involves the application of a cyclic low-velocity force. [6]
Similar to any medical intervention, joint manipulations and mobilizations are not without risk of harms or complications. [7] Whilst serious harms have been reported to be rare [8–11], the consequences of such can be devastating, with considerable impact on those involved. Patient safety remains a top priority within healthcare, with a continued focus on preventing and minimising adverse events following any type of intervention. [12, 13] A 2015 North American Patient Safety Foundation expert panel emphasised the importance of patient safety as a public health issue with a main recommendation being the need for a common set of safety metrics for use across all practice settings, including primary or ambulatory care settings, which is where the majority of care is provided. [14, 15]
“Harms”, “complications”, “side-effects” and “adverse events” are among several commonly used terms in the literature describing undesirable outcomes of manual interventions (e.g., spinal and peripheral joint manipulation and mobilization), which are most commonly used to reduce pain and disability in patients with musculoskeletal complaints. [16–18] Additionally, how these outcomes are defined and what constitutes an adverse event (or undesirable outcome) following spinal and peripheral joint manipulation and mobilization remains disparate. [19–21]These outcomes may be further classified according to their severity (e.g., mild, moderate, severe), onset (e.g., during treatment, within 24–48 hours after treatment), duration (e.g., transient, short-lasting, permanent) or need for unplanned additional remedial or medical care (e.g., investigations, specialist referral, hospitalisation). [22, 23] The kaleidoscope of domains and descriptors used in the literature to report and characterize these outcomes impedes attempts to advance patient safety initiatives and practices through a common and universal understanding of observed safety incidents. Although previous studies have highlighted this issue [16] and proposed frameworks for categorizing adverse events following manual therapy [23–25], there is still no standardization as to what constitutes an adverse event following such manual therapy interventions. A standardized and accepted adverse event typology would not only facilitate the development of strategies to minimise or prevent such events across all manual therapy professions that use these interventions, but more importantly, achieve consistency and precision in documenting and reporting such events. Specifically, an adverse events typology should include an operational definition of an adverse event so that identification, reporting and learning opportunities can be standardized across professions using spinal and peripheral joint manipulation and mobilization.
For these reasons, a scoping review of the literature is required. Combining the published knowledge from different professions, healthcare settings and musculoskeletal conditions will elucidate the current landscape and true extent of the problem. Findings from this scoping review will provide the evidence needed to conduct further research and move towards a consensus on the topic of adverse events. Ultimately, enhancing patient safety practices for spinal and peripheral joint manipulation and mobilization.
Aim and objectives
This scoping review aimed to map the scientific literature defining adverse events and their respective classification systems following spinal or peripheral joint manipulation and mobilization for musculoskeletal conditions in an adult population.
Specific objectives included:
To describe how adverse events following spinal and peripheral joint manipulation and mobilization have been defined in the literature;
To describe how adverse events following spinal and peripheral joint manipulation and mobilization have been classified in the literature.
Materials and methods
Design
This scoping review followed the Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) for transparency in reporting. [26] The protocol was registered at the Open Science Framework Registry (10.17605/OSF.IO/UBX2D) and designed by an international, interprofessional team of manual therapists (chiropractors, osteopaths and physiotherapists) with relevant clinical and methodological expertise. A scoping review was chosen as this study focuses on examining and clarifying definitions and classification systems for adverse events following spinal and peripheral joint manipulation and mobilization that are used in the literature. [27]
Stages
This review was conducted in 5 stages:(1) identifying the research question;
(2) identifying relevant studies;
(3) study selection;
(4) charting the data; and
(5) collating, summarizing and reporting the results. [28, 29]The optional consultation exercise (step 6) was not included within the scope of this specific manuscript as the results will be used to inform an e-Delphi study. [30]
Stage 1: Identifying the research question How does the scientific literature define adverse events and their respective classification systems for events that occur following spinal or peripheral joint manipulation and mobilization for musculoskeletal conditions in an adult population?
Stage 2: Identifying relevant studies Information sources. The following databases were searched from inception to 12th February 2021: MEDLINE, EMBASE, CINAHL, Scopus, AMED, ICL, PEDro and Cochrane Library. Grey literature using Open Grey and Open Access Theses and Dissertations (OATD) were also searched.

Table 1 Search strategy. The search strategy was designed by the authors with the assistance of an experienced health sciences librarian. The initial search strategy (S1 Table) was developed for Ovid MEDLINE using medical subject headings (MeSH) and text words. This was subsequently adapted to the syntax and subject headings of the other databases that were searched.
Eligibility criteria. Studies were identified by using the eligibility criteria outlined in Table 1.For the purpose of this study, mobilization was defined as a manual therapy technique comprising a continuum of skilled passive movements that were applied at varying speeds and amplitudes to joints. [6] Manipulation was defined as a passive, high velocity, low amplitude thrust applied to a joint complex within its anatomical limit (the range of motion of the joint complex in which active and passive motion occurs and not beyond the joint’s anatomic limit). [6] The term “adverse event” was adopted as an umbrella term to reflect any undesirable effect of spinal or peripheral joint manipulation and mobilization where terms such as “harms”, “complications”, “side-effects”, etc. have also been used in the literature. [16–18]
Stage 3: Study selection This stage was conducted in 2 phases with each phase starting with a pre-screening team meeting to discuss inclusion and exclusion criteria. Both phases were performed using Covidence systematic review software (Veritas Health Innovation, Melbourne, Australia), an online tool developed for systematic reviews by the Cochrane Collaboration that follows the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guidelines. Five reviewers screened the same 20 publications to ensure inter-screener calibration with weekly meetings to resolve any conflicts. Specifically, in phase 1, titles and abstracts were independently screened by two of the five reviewers to identify potentially relevant studies. Any disagreements were resolved through discussion. Phase 2 was based on the full texts of all studies identified as potentially relevant during phase 1. Similar to phase 1, two of the five reviewers independently screened full texts and any disagreements were resolved by discussion and consensus with all five reviewers.
Stage 4: Charting the data Data were extracted by all five reviewers working as a group using a standardized data extraction form that was first piloted with 20 included studies. All data extracted were checked for accuracy by two reviewers (MF and LG). Disagreements were resolved through discussion and consensus.
Extracted data included study characteristics (first author, year of publication, title, country, study design [original studies: case report/series, observational studies, consensus, survey, experimental trials, other designs; and clinical practice guidelines, review or study protocols]), participant population for original studies or study protocol (sample size, condition being treated [spinal, peripheral, mixed, unknown, not applicable], condition severity, condition chronicity [acute (<3 weeks), subacute (>3 weeks, <3 months), chronic (>3 months), mixed, unknown]), studies description for clinical practice guidelines and review (number of included studies, design of included studies), intervention characteristics (setting [community-based clinic/office, hospital, research clinic, academic institute, mixed], profession [chiropractic, naprapathy, osteopathy, physiotherapy, mixed, other, unknown], intervention [manipulation, mobilization, mixed]), and adverse event characteristics (definition, classification system [e.g., minor-moderate-major; mild-moderate-severe-serious], citations for adverse event definitions or classification systems, and whether the provided adverse event definition was direct (a clear statement of what was considered an adverse event) or indirect (indicated what was considered an adverse event without a clear statement [e.g., provided the question asked to participants during the study])).
Stage 5: Collating, summarizing and reporting the results Extracted data were categorized into two groups: i) studies providing a direct definition and/or classification system for adverse events following spinal and peripheral joint manipulation or mobilization; and ii) studies providing an indirect definition and/or classification system for adverse events following these interventions. Specifically, studies providing a direct definition and/or classification were those that provided a clear statement of the study’s operational definition and/or classification system for adverse events. For example: “For the purposes of this study, we adopted the following definition (derived from the ICH Guidelines for Good Clinical Practice): An adverse event (AE) can be any unfavourable and unintended sign, symptom, or disease temporally associated with the use of an intervention (treatment), which does not necessarily have a causal relationship with such treatment”. [31] Studies providing an indirect definition and/or classification were those that did not provide a clear statement of their operational definition and/or classification system, but indicated what was considered an adverse event, for example, by providing the question used to collect adverse events in a survey. For example: “[…] possible adverse effects were assessed by 2 open-ended questions: (1) “Did your symptoms get worse after this treatment?” and (2) “Are you feeling any different symptoms after this treatment?”. [32] A descriptive summary detailing the overall number of studies included in the review, their study characteristics as well as the data regarding adverse event definition and classification system extracted from included studies are provided.
Results
Study selection
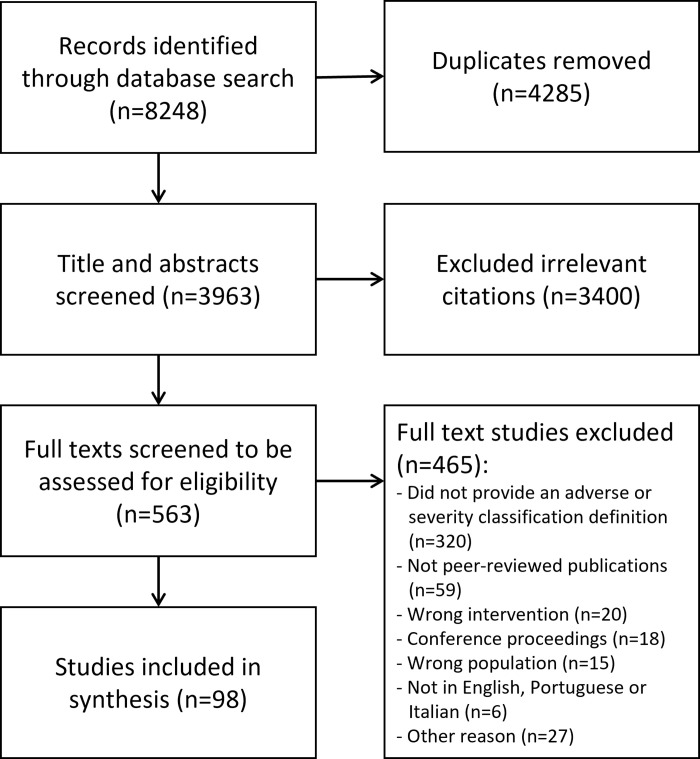
Figure 1 Electronic searches identified 8,248 citations that resulted in 3,963 unique citations to be screened for inclusion following the removal of duplicates. The titles and abstracts were assessed for their relevance to the review based on the eligibility criteria (phase 1 screening), where 3,400 citations were excluded, resulting in 563 citations for full text review. The phase 2 screening excluded 465 full texts: 320 did not provide an adverse event definition or classification, 59 were not peer-reviewed publications, 20 included the wrong intervention (e.g., did not use joint manipulation or mobilization), 18 were conference proceedings, 15 included the wrong population (e.g., participants younger than 18 or older than 65 years old), 6 were not written in English, Portuguese or Italian and 27 were excluded for other reasons (e.g., full text not available, professional issue papers, etc.). As such, 98 studies were included in this scoping review (Figure 1).
Characteristics of included studies
The 98 included studies were published between 1993 and 2021, mostly from North America (n = 42) and Europe (n = 36). Thirty-three studies focused on joint manipulation, 5 focused on mobilization and 60 included both techniques. Study settings mainly comprised academic institutes (n = 40) and provided manipulation or mobilization to the spine (n = 67). Study designs were: literature reviews (n = 21), surveys (n = 20), clinical trials (n = 18), observational studies (n = 10), protocols (n = 10), case report/series (n = 6), consensus studies (n = 5), clinical practice guidelines (n = 4), qualitative studies (n = 2), and “other” (n = 2) (e.g., retrospective analysis). A direct definition for an adverse event and/or classification system was provided in 69 studies, while 29 provided an indirect definition and/or classification system.
Data synthesis
Table 2
Table 3
Table 4 Studies with a direct adverse event definition and/or classification system
The studies that provided a direct definition of an adverse event and/or classification system (n = 69) were published between 1993 and 2020 and were mostly from North America (n = 28) and Europe (n = 27). Twenty-two studies focused on joint manipulation, 4 focused on mobilization and 43 included both techniques. Most were conducted in an academic institute (n = 26) and provided the intervention to the spine (n = 48).
Study designs included:surveys (n = 15),
reviews (n = 13),
trials (n = 12),
protocols (n = 9),
observational studies (n = 6),
consensus studies (n = 5),
case reports/series (n = 4),
clinical practice guidelines (n = 2) and
other designs (e.g., qualitative studies) (n = 3).Of these, 19 studies provided a direct definition of an adverse event only, 20 provided a classification system only, and 30 provided both a direct definition and classification system (Tables 2–4).
In addition to the term “adverse events”, the term “side-effects” was used in 4 studies, “sequelae” was used in 4 studies, “complication” in 3 studies, “incident” in 2 studies and one study used the term “reaction”. New or worsened complaints or symptoms were described as adverse events in 18 studies. Twenty studies described adverse events as “unpleasant”, “unfavourable”, “unintended”, “unexpected” and/or “undesired responses”, and 5 studies as “untoward medical occurrences”. Common descriptors composing the adverse event definition statements were identified in the studies that provided a direct definition of an adverse event (n = 49). Specifically, causality was incorporated in the definition provided by 21 studies (e.g., “Adverse events are unexpected events […] without evidence of causality” [33]). Symptom severity was used to define adverse events in 20 studies (e.g., “Adverse events are moderate to severe […]” [34]). Symptom onset was included in the definition provided by 19 studies (e.g., “Adverse events were events that occurred within 24 hours following the treatment” [19]). Symptom duration was used as a descriptor in 10 studies (e.g., “[…] increased pain and/or stiffness of short duration” [35]). In general, studies including chiropractors defined adverse events as an “unpleasant reaction” or “new or worsened symptom” more often than studies including other professions.
Among the studies that provided a classification system (n = 50), 23 only described the end anchors of the classification (e.g., mild/minor and/or serious), 26 provided description of additional classification categories (e.g., moderate, severe, etc.) and 3 described a classification system not including severity (e.g., common and uncommon; preventable and not preventable). Common domains that were used to describe the severity classification categories included: intensity (e.g., “We classified adverse event intensity as NRS score of 1 to 3 = mild, score of 4 to 6 = moderate; and NRS score of 7 to 10 = severe” [47]); duration (e.g., mild = less than 24 hours, moderate = between 24 hours and 1 week, major = over 1 week [24]); functional impact (e.g., mild = function intact, moderate = function modified, major = function impaired [79]); and requirement of additional treatment (e.g., mild = no additional intervention, moderate = may need additional intervention, severe = required intensive intervention [55]). Overall, studies conducted in Asia classified adverse events according to the Spilker classification [90] more often than those conducted in other regions.
Table 5 Among the 69 studies that provided a direct definition and/or classification system, 56 cited a reference or a source for the definition used, while 13 did not provide any reference or source. In total, 78 unique references were cited of which 55 were peer-reviewed publications and 23 were books, websites, online documents or other sources (Table 5).
While most of the references were related to manual therapy (n = 46), studies and sources from other areas (e.g., oncology, pharmacology) and organizations (e.g., Agency for Healthcare Research and Quality, World Health Organization, National Patient Safety Agency) were also referenced (n = 29). Generally, studies including chiropractors cited Senstad et al. (1996a, 1996b, 1997) [36, 57, 91] more often than other professions; and studies including physiotherapists cited Carnes et al. (2010a) [23] and Carlesso et al. (2010, 2011) [16, 79] more often than other professions. Additionally, studies conducted in North America often referenced studies by Carnes et al. (2010a) [23] and Carlesso et al. (2010, 2011) [16, 79]; studies conducted in Europe often cited Carnes et al. (2010a, 2010b) [23, 92], Carlesso et al. (2010) [16], Senstad et al. (1997) [57], and Cagnie et al. (2004) [93]; and studies conducted in Asia referenced work from Spilker et al. (1991) [90] (S2 Table).
Studies with an indirect adverse event definition and/or classification system
Table 6
Table 7
Table 8 The studies that provided an indirect definition of an adverse event and/or classification system (n = 29) were published between 1996 and 2021, mostly from North America (n = 14) and The United Kingdom (n = 6). Eleven studies focused on spinal and/or peripheral joint manipulation, 1 focused on mobilization and 17 included both techniques. Most were conducted in an academic institute (n = 14) and provided manipulation or mobilization to the spine (n = 19).
Study designs included:reviews (n = 8),
trials (n = 6),
surveys (n = 5),
observational studies (n = 4),
clinical practice guidelines (n = 2),
case reports/series (n = 2), protocol (n = 1) and
qualitative study (n = 1).Of these 29 studies, 4 provided an indirect definition of an adverse event only, 10 provided a classification system only, and 15 provided both an indirect definition and classification system (Tables 6–8).
Indirect definitions commonly referred to adverse events as “new or worsening symptoms” (e.g., “One adverse reaction (an exacerbation of pain after the initial assessment) was recorded.” [94]). The most commonly used categories used to classify adverse events were words such as “minor”, “mild”, “moderate”, “serious” and “severe” (e.g., “[…] adverse events were mild to moderate, self-limiting, and reported by 30% of patients […]” [95]). Common domains that were used to indirectly describe the severity classification categories included: onset (e.g., “Most of these AEs [adverse events] occurred within 4 hours of SMT [spinal manipulative therapy]” [96]); duration (e.g., “If the subjects indicated that they had experienced any side effect, then they were asked to report […], the duration (categorized as ≤24 hours or ≥24 hours) […]” [97]); and/or action taken (e.g., “There was no record of interrupted treatment due to side effects” [91]).
Table 9 Among the 29 studies that provided an indirect definition and/or classification system, 14 cited a reference or a source for the definition used, while 15 did not. In total, 27 unique references were cited among which 24 were peer-reviewed publications and 3 were books, websites, online documents or other sources (Table 9). Most of the references were related to manual therapy, including spinal and peripheral joint manipulation and mobilization, (n = 20); however, other areas (e.g., aviation) and sources (e.g., clinical practice guideline, dictionary) were also cited (n = 7).
Discussion
This study mapped the scientific literature discussing the definition of adverse events and their classification systems following spinal and peripheral joint manipulation and mobilization for musculoskeletal conditions in an adult population. Based on the 98 included studies, heterogeneous adverse event definitions and classification systems were identified. This empirical evidence of heterogeneity highlights the need for international and interprofessional consensus on a standardized definition and classification system so that patient safety practices for spinal and peripheral joint manipulation and mobilization can be more homogeneous, facilitating synthesis of findings and outcomes and, consequently, improving patient care.
Definition components
Despite adverse events following spinal and peripheral joint manipulation and mobilization being investigated since the 1990s, a clear definition and classification system has yet to be established. Our findings highlight that even the terms used to refer to adverse events vary, ranging from “side effects” to “symptomatic responses” to “harms”, “complications”, “adverse response/reaction/effects/events/ experience”, among others. [36, 42, 45, 48, 66, 71, 91]
Given the importance of this topic and the increased focus of healthcare on patient safety [13], it is surprising that the standardization of terms, definition and classification system have not yet been established. This, in turn, could have contributed to the lack of adverse event reporting systems within professions that use joint manipulation and mobilization interventions. An established reporting system that accurately collects the number of spinal and peripheral joint manipulations and mobilizations delivered [120] would allow more precise estimations of the incidence of adverse events following these interventions and potential contributing factors to such events could be investigated.
Our findings identified descriptors commonly used to define adverse events and classification systems: causality, symptom severity, onset and duration, and action taken. Establishing causality between the delivery of a manual intervention and an adverse event is challenging. This relationship/association has long been a discussion within manual therapy [23, 121, 122], other healthcare arenas [123–127] and the overall field of patient safety. [18, 128] Recently, a tool to assess causality of adverse events associated with any therapeutic interventions has been developed that could assist with this complex issue. [129] In addition to being one of many components of adverse event definitions identified in this study, this standardized tool to assess causality may assist with the identification of predisposing factors which, in turn, could contribute to the development of prevention and mitigation strategies of similar adverse events. [130] Therefore, a standardized operational definition for what constitutes an adverse event is needed to allow for the identification of adverse events across professions and this tool could be used to assess the causality of accurately identified adverse events.
Symptom severity (or intensity), onset and duration, and action taken (e.g., medication use, seeking unplanned medical care) were descriptors commonly used to define both what constitutes an adverse event and describe the classification system categories (Tables 2–4). For example, symptom severity was observed within adverse event definitions when it included the worsening and aggravation of a symptom (e.g., increased pain). Additionally, adverse events were classified as minor (or mild), moderate or major (or severe) based on the symptom duration, with minor (or mild) adverse events being short-duration (e.g., less than 24 hours) and major (or severe) adverse events being long term. Although different studies used different thresholds (e.g., considering short duration 24 or 48 hours), these descriptors were observed in most included studies.
Overall, in healthcare, adverse events have been classified based on theintervention (e.g., vaccine adverse event),
anatomical location (e.g., eye adverse event),
severity (e.g., serious adverse event), or
causality (e.g., causal adverse event). [18]However, specific classifications within medical areas have been developed to better characterize adverse events, contributing to advancements within patient safety by enabling better synthesis of information. [131–134] For example, Kaafarani et al. (2014) proposed that the classification of intraoperative adverse events to range from Class I (injury requiring no repair with the same procedure) to Class VI (intraoperative). [134] Kaufman (2016) identified that not all adverse drug reactions fit into the previously established types A (predictable) and B (novel responses) and proposed the addition of type C (continuing), type D (delayed use) and type E (end of use) reactions. [133] Therefore, developing a standardized classification specific for adverse events following spinal and peripheral joint manipulation and mobilization could provide a common language for all professions that use these interventions and facilitate identification, reporting and communication about adverse events, promoting interprofessional learning and contributing to advancing patient safety.
Multidisciplinarity
Although adverse events following spinal and peripheral joint manipulation and mobilization have been the focus of several studies, these often include one profession (e.g., chiropractic, naprapathy, osteopathy, physiotherapy, etc.). [19, 31, 47, 60] Given the number of professions using these manual therapy interventions, it is possible that the inter-professional knowledge exchange related to definitions and classification of adverse events was limited as each profession focused on their individual (siloed) professional communities rather then the intervention at large. Indeed, this review identified that included studies tended to cite references that were published by authors in the same profession. Although communication across health-related professions has been observed to be well-established and a common practice among academic communities [135, 136], joint manipulation and mobilization providers have been described to present an unique culture related to patient safety. [137]
Specifically, divergent intra- and inter-profession beliefs, overlapping scopes of practice and perceived business competition may prevent interprofessional communications focused on adverse events following these interventions. [137] However, in order to advance joint manipulation and mobilization safety initiatives, enhanced interprofessional communications and collaborations are not only possible but fundamental. We have attempted to address this issue by establishing an international, multidisciplinary working group investigating adverse event definition and classification systems across all professions using joint manipulation and mobilization. Another example includes the international framework for risk assessment of cervical artery dysfunction [138], which included a multidisciplinary research team.
Furthermore, in 2010a, Carnes and colleagues conducted a multidisciplinary Delphi study with the aim to seek an expert consensus definition for adverse events applicable to all professions that use manual therapy. [23] Similarly, Carlesso et al. (2011) explored how patients receiving manual therapy from different professions defined adverse events. [79] These are two of the few multidisciplinary studies, including different professions (i.e., chiropractic, osteopathy, physiotherapy) that use spinal and peripheral joint manipulation and mobilization and were referenced by 19% and 7% of the 98 included studies in this scoping review, respectively. This percentage of referencing is slightly lower than the average 20%–35% interprofessional referencing in medical sciences [136] and could potentially explain, at least partially, the heterogenous adverse event definition and classification systems observed in this study.
Although Carnes et al. (2010a) did not achieve consensus on a succinct adverse event definition, a proposed classification system was clearly determined and described. [23] Remarkably, even though this work was published over a decade ago, the definition of an adverse event and their classification systems remained noticeably heterogeneous in the manual therapy literature, including in studies published after Carnes et al. (2010a). This reinforces the possibility of limited interprofessional knowledge exchange related to this specific topic, and the importance of the broad dissemination of results going beyond individual professions, as well as efforts from all professions to enhance interprofessional, topic-related knowledge, rather than profession-specific.
Geography
The heterogeneity in adverse event definitions and classification systems identified in this study could potentially be due to the fact that spinal and peripheral joint manipulation and mobilization are interventions commonly used by different professionals located in different geographical locations. [139–141] Variation in professions’ scope of practice and regulations between continents, countries and even regional jurisdictions could lead providers to use their own definition for an adverse event, based on their local practices and regulations. [139, 142] Additionally, the emergence of litigation most commonly related to serious adverse events following manipulation leading to significant disability, such as vertebral artery dissection, cauda equina syndrome, etc., may have contributed to the development of local definitions. [11, 21, 80, 104] As the number of serious and life-threatening adverse events reports following manipulation increased, so did the number of malpractice lawsuits against professionals who use these interventions. [143–145] Consequently, legal courts, lawyers and malpractice insurers were likely compelled to develop local definitions in order to process and rule on such cases. Given that any practising provider is vulnerable to experiencing malpractice lawsuits against them, they may feel bound to these local definitions to be consistent with the environment in which they practice.
Additionally, given the diverse geographical locations in which spinal and peripheral joint manipulation and mobilization are used, cultural differences and their influence on individual beliefs and behaviours could also be a potential contributor to the adverse event definition and classification system heterogeneity found in this study. [146] Culture refers to values, norms, and codes that collectively shape the beliefs, attitudes, and behavior of a group. [147] Indeed, the impact of culture on health has been widely investigated as better understanding cultural contexts advances the knowledge of inter-personal roles, connections, and relationships (whether positive or negative), as well as allowing the understanding of how individuals are shaped and their health. [147–150] Consequently, cultural differences can play an important role in how adverse events after these interventions are defined and classified and may have a significant contribution to the heterogeneity identified in this study.
This review identified trends in citations where specific continents used specific references more often in comparison to other continents. Besides demonstrating a potential limitation in knowledge exchange across geographical locations, this finding highlights the paucity of studies related to this topic from some parts of the world, including Africa and South America. Therefore, including these continents when developing a standardized adverse event definition and classification system is of great importance not only to take into consideration geographical and cultural particularities, but also to support the development of investigations related to this topic in these locations.
Future studies
Based on these findings, an e-Delphi study will be conducted to establish a standardized adverse event definition and classification system that can be prospectively used across multiple professions. [30] This has the potential to greatly advance patient safety as it would provide a standardized framework for data to be collected and synthesized in an uniform manner. This would then provide all stakeholders of spinal and peripheral joint manipulation and mobilization interventions a comprehensive patient safety profile for the adult population with musculoskeletal conditions. Insights gained from this profile could assist with the formation and streamlining of clinical guidelines and further research capacities.
Strengths and limitations
Strengths of this study include the involvement of an interprofessional research group with clinical and methodological expertise, and development of the protocol a priori for transparency. Additionally, this review was not limited by country or profession; therefore, our findings are representative and transferable to an international and interprofessional audience.
Although the search included several potential terms related to adverse events, it is possible that potentially relevant studies that used alternate terms to describe adverse events were not captured. The search was also limited to studies published in English, Italian and Portuguese languages; potentially relevant studies published in other languages (such as German, French, Dutch, etc.) were not captured. Additionally, adverse event definitions provided by included studies were categorized into “direct” and “indirect”. Although this categorization was clearly defined (i.e., direct definition provided a clear statement of what was considered an adverse event; indirect definition indicated what was considered an adverse event without a clear statement [e.g., provided the question asked to participants during the study]), it is not an established categorization and contains some level of subjectivity.
Conclusion
Findings identified that a vast array of terms, definitions and classification systems for adverse events following spinal and peripheral joint manipulation and mobilization have been published. Within this array of literature, there was no one standardized adverse event definition or classification system for adverse events following these interventions that is commonplace and widely used. This suggests that establishing a consensus on standardized terms, definitions and classification systems for adverse events related to these interventions is urgently needed and could advance strategies to enhance patient safety for all professions who deliver these interventions.
Supporting information
S1 Checklist
Preferred Reporting Items for Systematic reviews and Meta-Analyses
extension for Scoping Reviews (PRISMA-ScR) checklist. (84K, docx)
S1 Table
The initial search strategy developed for Ovid MEDLINE. (34K, pdf)
S2 Table
Citation by geographical location. (17K, docx)Acknowledgements
The authors would like to acknowledge Dr. Martina Gosteli (University of Zürich) for her assistance with the search strategy used in this study and conducting database searches, as well as Ms. Gloria Field and Mr. Zak Monier (Parker University) for their assistance with retrieving full texts for this study.
Funding Statement
The authors received no specific funding for this work.
References:
James SL, Abate D, Abate KH, Abay SM, Abbafati C, Abbasi N, et al.
Global, regional, and national incidence, prevalence, and years lived with
disability for 354 diseases and injuries for 195 countries and territories,
1990–2017: a systematic analysis for the Global Burden of Disease Study 2017.
Lancet. 2018;392: 1789–1858.
doi: 10.1016/S0140-6736(18)32279-7Cieza A, Causey K, Kamenov K, Hanson SW, Chatterji S, Vos T.
Global estimates of the need for rehabilitation based on the Global Burden
of Disease study 2019: a systematic analysis for
the Global Burden of Disease Study 2019.
Lancet. 2020;6736: 1–12. doi:
10.1016/S0140-6736(20)32340-0Lin I, Wiles L, Waller R, Goucke R, Nagree Y, Gibberd M, et al.
What Does Best Practice Care for Musculoskeletal Pain Look Like?
Eleven Consistent Recommendations From High-quality
Clinical Practice Guidelines: Systematic Review
British J Sports Medicine 2020 (Jan); 54 (2): 79–86Hawk C, Whalen W, Farabaugh RJ, et al.
Best Practices for Chiropractic Management of Patients with
Chronic Musculoskeletal Pain: A Clinical Practice Guideline
J Altern Complement Med 2020 (Oct); 26 (10): 884–901National Institute for Health and Care Excellence (NICE):
Low Back Pain and Sciatica in Over 16s:
Assessment and Management (PDF)
NICE Guideline, No. 59 2016 (Nov): 1–1067Rushton Karen; Beeton Ronel; Jordaan John Langendoen; Lenerdene Levesque; et al.
Educational Standards In Orthopaedic Manipulative Therapy. 2016; 91. Available:
http://www.ifompt.org/site/ifompt/IFOMPTStandardsDocumentdefinitive2016.pdfMarra AR, Algwizani A, Alzunitan M, Brennan TMH, Edmond MB.
Descriptive epidemiology of safety events at an academic medical center.
Int J Environ Res Public Health. 2020;17: 1–11.
doi: 10.3390/ijerph17010353Powell FC, Hanigan WC, Olivero WC.
A risk/benefit analysis of spinal manipulation therapy for relief
of lumbar or cervical pain.
Neurosurgery. 1993;33: 73–79. Available:
http://ovidsp.ovid.com/ovidweb.cgi?T=JS&PAGE=reference&D=med3&NEWS=N&AN=8355850
doi: 10.1227/00006123-199307000-00011Rubinstein SM, Leboeuf-Yde C, Knol DL, de Koekkoek TE,
Pfeifle CE, van Tulder MW.
The Benefits Outweigh the Risks for Patients Undergoing Chiropractic
Care for Neck Pain A Prospective, Multicenter, Cohort Study
J Manipulative Physiol Ther 2007 (Jul); 30 (6): 408–418Degenhardt BF, Johnson JC, Brooks WJ, Norman L.
Characterizing Adverse Events Reported Immediately
After Osteopathic Manipulative Treatment.
J Am Osteopath Assoc. 2018;118: 141–149.
doi: 10.7556/jaoa.2018.033Swait G, Finch R.
What Are the Risks of Manual Treatment of the Spine?
A Scoping Review for Clinicians
Chiropractic & Manual Therapies 2017 (Dec 7); 25: 37Kohn LT, Corrigan JM, Donaldson M, eds.
To Err Is Human: Building a Safer Health System
Washington, DC: Institute of Medicine (Nov 1999)WHO (World Health Organization)
Towards Eliminating Avoidable Harm in Health Care
Draft Global Patient Safety Action Plan 2021-2030, 2021.Foundation NPS.
Free from Harm: Accelerating Patient Safety Improvement
Fifteen Years after To Err Is Human.
Boston, MA. 2015. doi:
10.5860/choice.43sup-0367Statistics NC for H.
FastStats A to Z. In:
https://www.cdc.gov/nchs/fastats/
[Internet]. 2015. [cited 26 May 2018].
doi: 10.5860/choice.36sup-305Carlesso LC, Macdermid JC, Santaguida LP.
Standardization of adverse event terminology and reporting in orthopaedic
physical therapy: application to the cervical spine.
J Orthop Sports Phys Ther. 2010;40: 455–463.
doi: 10.2519/jospt.2010.3229Gorrell LM, Engel RM, Brown B, Lystad RP.
The reporting of adverse events following spinal manipulation
in randomized clinical trials-a systematic review.
Spine J. 2016;16: 1143–1151.
doi: 10.1016/j.spinee.2016.05.018He Y, Sarntivijai S, Lin Y, Xiang Z, Guo A, Zhang S, et al.
OAE: The Ontology of Adverse Events.
J Biomed Semantics. 2014;5: 1–13.
doi: 10.1186/2041-1480-5-29Paanalahti K, Holm LW, Nordin M, Asker M, Lyander J, Skillgate E.
Adverse events after manual therapy among patients seeking care for
neck and/or back pain: a randomized controlled trial.
BMC Musculoskelet Disord. 2014;15: 77.
doi: 10.1186/1471-2474-15-77Dougherty PE, Karuza J, Savino D, Katz P.
Evaluation of a Modified Clinical Prediction Rule For Use With
Spinal Manipulative Therapy in Patients With Chronic Low
Back Pain: A Randomized Clinical Trial
Chiropractic & Manual Therapies 2014 (Nov 18); 22 (1): 41Nielsen SM, Tarp S, Christensen R, Bliddal H, Klokker L, Henriksen M.
The risk associated with spinal manipulation: an overview of reviews.
Syst Rev. 2017;6: 64.
doi: 10.1186/s13643-017-0458-yPohlman KA, Beirne MO, Thiel H, Cassidy JD, Mior S, Hurwitz EL, et al.
Development and Validation of Providers’ and Patients’
Measurement Instruments to Evaluate Adverse Events
After Spinal Manipulation Therapy
Eur J Integr Med. 2014 (Aug); 6 (4): 451–466Carnes D, Mullinger B, Underwood M.
Defining adverse events in manual therapies: A modified delphi consensus study.
Int J Osteopath Med. 2010;13: 94–98.
doi: 10.1016/j.math.2009.02.003Carlesso LC, Macdermid JC, Santaguida PL, Thabane L.
Determining adverse events in patients with neck pain receiving orthopaedic
manual physiotherapy: a pilot and feasibility study.
Physiother Can. 2013;65: 255–265.
doi: 10.3138/ptc.2012-28Carlesso LC, Macdermid JC, Santaguida PL, Thabane L.
A survey of patient’s perceptions of what is “adverse” in manual physiotherapy
and predicting who is likely to say so.
J Clin Epidemiol. 2013;66: 1184–1191.
doi: 10.1016/j.jclinepi.2013.05.005Tricco AC, Lillie E, Zarin W, O’Brien KK, Colquhoun H, Levac D, et al.
PRISMA Extension for Scoping Reviews (PRISMA-ScR):
Checklist and Explanation.
Ann Intern Med. 2018;169: 467–473.
doi: 10.7326/M18-0850Munn Z, Peters MDJ, Stern C, Tufanaru C, McArthur A, Aromataris E.
Systematic review or scoping review? Guidance for authors when
choosing between a systematic or scoping review approach.
BMC Med Res Methodol. 2018;18: 1–7.
doi: 10.1186/s12874-018-0611-xArksey H, O’Malley L.
Scoping studies: Towards a methodological framework.
Int J Soc Res Methodol Theory Pract. 2005;8: 19–32.
doi: 10.1080/1364557032000119616Levac D, Colquhoun H, O’Brien KK.
Scoping studies: advancing the methodology.
Implement Sci. 2010;5: 69.
doi: 10.1186/1748-5908-5-69Funabashi M, Pohlman KA, Gorrell LM, Salsbury SA, Bergna A, Heneghan NR.
Severity Classification for Adverse Events Associated with
Spinal and Peripheral Joint Manipulation and Mobilisation:
Protocol for an International E-Delphi Study
BMJ Open 2021 (Nov 11); 11 (11): e050219Rajendran D, Mullinger B, Fossum C, Collins P, Froud R.
Monitoring self-reported adverse events: a prospective,
pilot study in a UK osteopathic teaching clinic.
Int J Osteopath Med. 2009;12: 49–55.
doi: 10.1016/j.ijosm.2008.08.031de Oliveira RF, Liebano RE, Costa L da CM, Rissato LL, Costa LOP.
Immediate effects of region-specific and non-region-specific
spinal manipulative therapy in patients with chronic low
back pain: a randomized controlled trial.
Phys Ther. 2013;93: 748–56.
doi: 10.2522/ptj.20120256Kranenburg HA, Lakke SE, Schmitt MA, Van der Schans CP.
Adverse events following cervical manipulative therapy:
consensus on classification among Dutch medical
specialists, manual therapists, and patients.
J Man Manip Ther. 2017;25: 279–287.
doi: 10.1080/10669817.2017.1332556Heneghan NR, Puentedura EJ, Arranz I, Rushton A.
Thoracic thrust joint manipulation: An international survey
of current practice and knowledge in IFOMPT member countries.
Musculoskelet Sci Pract. 2020;50: 102251.
doi: 10.1016/j.msksp.2020.102251O’Shaughnessy J, Drolet M, Roy J-FF, Descarreaux M, O J., D M., et al.
Chiropractic management of patients post-disc arthroplasty:
Eight case reports.
Chiropr Osteopat. 2010;18: 7.
doi: 10.1186/1746-1340-18-7Senstad O, Leboeuf-Yde C, Borchgrevink C.
Predictors of side effects to spinal manipulative therapy.
J Manipulative Physiol Ther. 1996. a;19: 441–445. Available:
http://ovidsp.ovid.com/ovidweb.cgi?T=JS&PAGE=reference&D=med4&NEWS=N&AN=8890024Leboeuf-Yde C, Hennius B, Rudberg E, Leufvenmark P, Thunman M.
Side effects of chiropractic treatment: a prospective study.
J Manipulative Physiol Ther. 1997;20: 511–515. Available:
http://ovidsp.ovid.com/ovidweb.cgi?T=JS&PAGE=reference&D=med4&NEWS=N&AN=9345679Thiel H, Bolton J.
The reporting of patient safety incidents—first experiences
with the Chiropractic Reporting and Learning System (CRLS):
a pilot study.
Clin Chiropr. 2006;9: 139–149.
doi: 10.1016/j.clch.2006.04.002Rubinstein SM, Knol DL, Leboeuf-Yde C, van Tulder MW.
Benign Adverse Events Following Chiropractic Care for
Neck Pain Are Associated With Worse Short-term
Outcomes but Not Worse Outcomes at Three Months
Spine (Phila Pa 1976) 2008 (Dec 1); 33 (25): E950–956Rubinstein SM, Leboeuf-Yde C, Knol DL, de Koekkoek TE, Pfeifle CE, van Tulder MW, et al.
Predictors of adverse events following chiropractic care
for patients with neck pain.
J Manipulative Physiol Ther. 2008;31: 94–103.
doi: 10.1016/j.jmpt.2007.12.006Wangler M, Fujikawa R, Hestbæk L, Michielsen T, Raven TJ, Thiel HW, et al.
Creating European guidelines for Chiropractic Incident Reporting
and Learning Systems (CIRLS): relevance and structure.
Chiropr Man Therap. 2011;19: 1–10.
doi: 10.1186/2045-709X-19-9Eriksen K, Rochester RP, Hurwitz EL.
Symptomatic Reactions, Clinical Outcomes and Patient
Satisfaction Associated with Upper Cervical
Chiropractic Care: A Prospective,
Multicenter, Cohort Study
BMC Musculoskelet Disord. 2011 (Oct 5); 12: 219Puentedura EJ, Landers MR, Cleland JA, Mintken PE, Huijbregts P, et al.
Thoracic spine thrust manipulation versus cervical spine thrust
manipulation in patients with acute neck pain:
A randomized clinical trial.
J Orthop Sports Phys Ther. 2011;41: 208–220.
doi: 10.2519/jospt.2011.3640Rubinstein SM, van Middelkoop M, Assendelft WJJJ, de Boer MR, et al.
Spinal manipulative therapy for chronic low-back pain.
Cochrane Database Syst Rev. 2011;36: CD008112.
10.1002/14651858.CD008112.pub2Dagenais S, Brady O, Haldeman S.
Shared decision making through informed consent in
chiropractic management of low back pain.
J Manipulative Physiol Ther. 2012;35: 216–226.
doi: 10.1016/j.jmpt.2012.01.004Nee RJ, Vicenzino B, Jull GA, Cleland JA, Coppieters MW.
Neural tissue management provides immediate clinically relevant
benefits without harmful effects for patients with nerve-related
neck and arm pain: a randomised trial.
J Physiother. 2012;58: 23–31.
doi: 10.1016/S1836-9553(12)70069-3Walker, BF, Hebert, JJ, Stomski, NJ et al.
Outcomes of Usual Chiropractic.
The OUCH Randomized Controlled Trial of Adverse Events
Spine (Phila Pa 1976). 2013 (Sep 15); 38 (20): 1723–1729Han L, Zhao P, Guo W, Wei J, Wang F, Fan Y, et al.
Short-term study on risk-benefit outcomes of two spinal manipulative
therapies in the treatment of acute radiculopathy caused by lumbar
disc herniation: study protocol for a randomized controlled trial.
Trials. 2015;16: 122.
doi: 10.1186/s13063-015-0634-0Woodfield HC III, York C, Rochester RP, Bales S, Beebe M, Salminen B, et al.
Craniocervical chiropractic procedures—a précis of
upper cervical chiropractic.
J Can Chiropr Assoc. 2015;59: 173–192. Available:
http://search.ebscohost.com/login.aspx?direct=true&db=rzh&AN=109814589&site=ehost-liveKim K, Shin K, Lee J-H, Seo B, Jung S, Youn Y, et al.
Nonsurgical Korean Integrative Treatments for Symptomatic Lumbar
Spinal Stenosis: A Three-Armed Randomized Controlled
Pilot Trial Protocol.
Evidence-based Complement Altern Med. 2016;2016: 2913248.
doi: 10.1155/2016/2913248Thoomes-de Graaf M, Thoomes EJ, Carlesso L, Kerry R, Rushton A.
Adverse effects as a consequence of being the subject of
orthopaedic manual therapy training, a worldwide
retrospective survey.
Musculoskelet Sci Pract. 2017;29: 20–27.
doi: 10.1016/j.msksp.2017.02.009Shin B-C, Kim M-R, Cho J-H, Jung J-Y, Kim K-W, Lee J-H, et al.
Comparative effectiveness and cost-effectiveness of Chuna manual
therapy versus conventional usual care for nonacute low back
pain: study protocol for a pilot multicenter, pragmatic
randomized controlled trial (pCRN study).
Trials. 2017;18: 26.
doi: 10.1186/s13063-016-1756-8Do HJ, Shin J-S, Lee J, Lee YJ, Kim M-R, Cho J-H, et al.
Comparative effectiveness and economic evaluation of Chuna
manual therapy for chronic neck pain: protocol for a
multicenter randomized controlled trial 11 Medical
and Health Sciences 1103 Clinical Sciences 11
Medical and Health Sciences 1117 Public Health.
Trials. 2018;19: 663. Available:
doi: 10.1186/s13063-018-3016-6Tabell V, Tarkka IM, Holm LW, Skillgate E.
Do adverse events after manual therapy for back and/or neck pain
have an impact on the chance to recover? A cohort study.
Chiropr Man Therap. 2019;27: 27.
doi: 10.1186/s12998-019-0248-9Lim K-T, Hwang E-H, Cho J-H, Jung J-Y, Kim K-W, Ha I-H, et al.
Comparative effectiveness of Chuna manual therapy versus
conventional usual care for non-acute low back pain:
a pilot randomized controlled trial.
Trials. 2019;20: 216.
doi: 10.1186/s13063-019-3302-yPohlman KA, Funabashi M, Ndetan H, Hogg-Johnson S, Bodnar P, Kawchuk G, et al.
Assessing Adverse Events After Chiropractic Care at a
Chiropractic Teaching Clinic: An Active-
Surveillance Pilot Study.
J Manipulative Physiol Ther. 2020;43: 845–854.
doi: 10.1016/j.jmpt.2020.05.007Senstad O, Leboeuf-Yde C, Borchgrevink C.
Frequency and characteristics of side effects of
spinal manipulative therapy.
Spine (Phila Pa 1976). 1997;22: 435–441.
doi: 10.1097/00007632-199702150-00017Malone DG, Baldwin NG, Tomecek FJ, Boxell CM, Gaede SE, Covington CG, et al.
Complications of cervical spine manipulation therapy: 5-year
retrospective study in a single-group practice.
Neurosurg Focus. 2002;13: ecp1.
doi: 10.3171/foc.2002.13.6.8Hurwitz EL, Morgenstern H, Vassilaki M, Chiang L-M.
Frequency and clinical predictors of adverse reactions to
chiropractic care in the UCLA neck pain study.
Spine (Phila Pa 1976). 2005;30: 1477–1484. Available:
http://ovidsp.ovid.com/ovidweb.cgi?T=JS&PAGE=reference&D=med6&NEWS=N&AN=15990659
doi: 10.1097/01.brs.0000167821.39373.c1Kuczynski JJ, Schwieterman B, Columber K, Knupp D, Shaub L, Cook CE.
Effectiveness of physical therapist administered spinal
manipulation for the treatment of low back pain:
a systematic review of the literature.
Int J Sports Phys Ther. 2012;7: 647–662. Available:
http://ovidsp.ovid.com/ovidweb.cgi?T=JS&PAGE=reference&D=pmnm2&NEWS=N&AN=23316428Puentedura EJ, March J, Anders J, Perez A, Landers MR, Wallmann HW, et al.
Safety of cervical spine manipulation: are adverse events
preventable and are manipulations being performed
appropriately? A review of 134 case reports.
J Man Manip Ther. 2012;20: 66–74.
doi: 10.1179/2042618611Y.0000000022Björklund M, Djupsjöbacka M, Svedmark Ĺ, Häger C.
Effects of tailored neck-shoulder pain treatment based on a
decision model guided by clinical assessments and
standardized functional tests. A study protocol
of a randomized controlled trial.
BMC Musculoskelet Disord. 2012;13.
doi: 10.1186/1471-2474-13-75Reid SA, Rivett DA, Katekar MG, Callister R.
Comparison of mulligan sustained natural apophyseal glides and
maitland mobilizations for treatment of cervicogenic
dizziness: a randomized controlled trial.
Phys Ther. 2014;94: 466–476.
doi: 10.2522/ptj.20120483MacPherson H, Newbronner E, Chamberlain R, Hopton A.
Patients’ experiences and expectations of chiropractic care:
a national crosssectional survey.
Chiropr Man Therap. 2015;23: 3.
doi: 10.1186/s12998-014-0049-0Rajendran D, Bright P, Mullinger B, Froud R.
Reporting patterns and predictors of common minor adverse events
following osteopathic treatment: Lessons learned from a
prospective, patient-administered questionnaire
feasibility study in a UK teaching clinic.
Eur J Integr Med. 2015;7: 634–644.
10.1016/j.eujim.2015.09.005Puentedura EJ, O’Grady WH.
Safety of thrust joint manipulation in the thoracic spine:
a systematic review.
J Man Manip Ther. 2015;23: 154–161. Available:
http://ovidsp.ovid.com/ovidweb.cgi?T=JS&PAGE=reference&D=pmnm3&NEWS=N&AN=26309386
doi: 10.1179/2042618615Y.0000000012Petrozzi MJ, Leaver A, Jones MK, Ferreira PH, Rubinstein SM, Mackey MG.
Does an online psychological intervention improve self-efficacy
and disability in people also receiving Multimodal Manual
Therapy for chronic low back pain compared to Multimodal
Manual Therapy alone? Design of a randomized controlled trial.
Chiropr Man Ther. 2015;23: 1–8.
doi: 10.1186/s12998-015-0080-9Bussičres AE , Stewart G , Al-Zoubi F , et al .
The Treatment of Neck Pain–Associated Disorders and
Whiplash-Associated Disorders:
A Clinical Practice Guideline
J Manipulative Physiol Ther 2016 (Oct); 39: 523–64Kranenburg HA, Schmitt MA, Puentedura EJ, Luijckx GJ, van der Schans CP.
Adverse events associated with the use of cervical spine
manipulation or mobilization and patient characteristics:
A systematic review.
Musculoskelet Sci Pract. 2017;28: 32–38.
doi: 10.1016/j.msksp.2017.01.008Heneghan NR, Davies SE, Puentedura EJ, Rushton A.
Knowledge and pre-thoracic spinal thrust manipulation examination:
a survey of current practice in the UK.
J Man Manip Ther. 2018;26: 301–309.
doi: 10.1080/10669817.2018.1507269Coulter ID, Crawford C, Hurwitz EL, Vernon H, Khorsan R, Suttorp Booth M, Herman PM.
Manipulation and Mobilization for Treating Chronic Low
Back Pain: A Systematic Review and Meta-analysis
Spine J. 2018 (May); 18 (5): 866–879Mikhail J, Funabashi M, Descarreaux M, Pagé I.
Assessing forces during spinal manipulation and mobilization:
factors influencing the difference between forces at the
patient-table and clinician-patient interfaces.
Chiropr Man Therap. 2020;28: 57.
doi: 10.1186/s12998-020-00346-1Stern PJ, Cote P, Cassidy JD.
A series of consecutive cases of low back pain with radiating
leg pain treated by chiropractors.
J Manipulative Physiol Ther. 1995;18: 335–342. Available:
http://ovidsp.ovid.com/ovidweb.cgi?T=JS&PAGE=reference&D=med3&NEWS=N&AN=7595106Hendry L, Yardley K, Hurley L, AR G.
Agreement of physiotherapists with advanced training in manual
therapy on magnitude of adverse events following the
application of cervical spine manual therapy.
Physiother Canada. 2002;54: 199–205. Available:
http://search.ebscohost.com/login.aspx?direct=true&db=rzh&AN=106852215&site=ehost-liveUnderwood M, UK BEAM Trial Team.
United Kingdom Back Pain Exercise and Manipulation (UK BEAM)
Randomized Trial: Effectiveness of Physical Treatments
for Back Pain in Primary Care
British Medical Journal 2004 (Dec 11); 329 (7479): 1377–1384Gibbons P, Tehan P.
HVLA thrust techniques: what are the risks?
Int J Osteopath Med. 2006;9: 4–12.
10.1016/j.ijosm.2006.02.005Thiel HW, Bolton JE, Docherty S, Portlock JC:
Safety of Chiropractic Manipulation of the Cervical Spine:
A Prospective National Survey
Spine (Phila Pa 1976). 2007 (Oct 1); 32 (21): 2375–2378Michael T Haneline, Robert Cooperstein.
Chiropractic care for patients with acute neck pain:
results of a pragmatic practice-based feasibility study.
J Chiropr Med. 2009;8: 143–155.
doi: 10.1016/j.jcm.2009.08.003Carlesso LC, Cairney J, Dolovich L, Hoogenes J.
Defining adverse events in manual therapy: An exploratory
qualitative analysis of the patient perspective.
Man Ther. 2011;16: 440–446.
doi: 10.1016/j.math.2011.02.001Hebert JJ, Stomski NJ, French SD, et al.
Serious Adverse Events and Spinal Manipulative Therapy
of the Low Back Region: A Systematic Review of Cases
J Manipulative Physiol Ther 2015 (Nov); 38 (9): 677–691Keating L.
A Randomised Controlled Trial of Multimodal Physiotherapy
for Patients With Acute / Sub-acute Cervical Radiculopathy.
In: Clinical Trials.gov [Internet]. 2015. [cited 16 Sep 2021]. Available:
https://clinicaltrials.gov/ct2/show/NCT02449200#wrapperKressig M, Peterson CK, McChurch K, Schmid C, Leemann S, Anklin B, et al.
Relationship of Modic Changes, Disk Herniation Morphology,
and Axial Location to Outcomes in Symptomatic Cervical
Disk Herniation Patients Treated With High-Velocity,
Low-Amplitude Spinal Manipulation: A Prospective Study.
J Manipulative Physiol Ther. 2016;39: 565–575.
doi: 10.1016/j.jmpt.2016.08.004Lisi AJ, Salsbury SA, Hawk C, Vining RD, Wallace RB, Branson R, et al.
Chiropractic Integrated Care Pathway for Low Back Pain
in Veterans: Results of a Delphi Consensus Process
J Manipulative Physiol Ther. 2018 (Feb); 41 (2): 137–148Frydman A, Johnston R V, Smidt N, Green S, Buchbinder R.
Manual therapy and exercise for lateral elbow pain.
Cochrane Database Syst Rev. 2018.
doi: 10.1002/14651858.CD013042Smith D, Hoogenboom B.
Sideline Management of Acute Dislocation of the Glenohumeral
Joint—A Unique Approach to Athlete Self-Reduction.
Int J Sports Phys Ther. 2013;8: 80–83. Available:
http://search.ebscohost.com/login.aspx?direct=true&db=rzh&AN=87519058&site=ehost-liveYao M, Tang ZY, Cui XJ, Sun YL, Ye XL, Wang P, et al.
Shi-Style Cervical Mobilizations Versus Massage for Cervical
Vertigo: A Multicenter, Randomized, Controlled Clinical Trial.
J Altern Complement Med. 2020;26: 58–66.
doi: 10.1089/acm.2019.0113Gross AR, Kay TM, Kennedy C, Gasner D, Hurley L, Yardley K, et al.
Clinical practice guideline on the use of manipulation or
mobilization in the treatment of adults with
mechanical neck disorders.
Man Ther. 2002;7: 193–205.
doi: 10.1054/math.2002.0477Skelly AC, Chou R, Dettori JR, Turner JA, Friedly JL, et al.
Noninvasive Nonpharmacological Treatment for Chronic Pain:
A Systematic Review Update
Comparative Effectiveness Review Number 227
Rockville (MD): Agency for Healthcare Research and Quality (2020)Funabashi M, French SD, Kranenburg HAR, Hebert JJ.
Serious adverse events following lumbar spine mobilization
or manipulation and potential associated factors:
a systematic review protocol.
JBI Evid Synth. 2020;Publish Ah.
doi: 10.11124/JBIES-20-00129Spilker B.
Guide to Clinical Trials.
Philadelphia: Lippincott Williams & Wilkins; 1991.Senstad O, Leboeuf-Yde C, Borchgrevink CF.
Side-effects of chiropractic spinal manipulation:
Types frequency, discomfort and course.
Scand J Prim Health Care. 1996. b;14: 50–53.
doi: 10.3109/02813439608997068Carnes D, Mars TS, Mullinger B, Froud R, Underwood M.
Adverse events and manual therapy: a systematic review.
Man Ther. 2010;15: 355–363.
doi: 10.1016/j.math.2009.12.006Cagnie B, Vinck E, Beernaert A, et al.
How Common Are Side Effects of Spinal Manipulation
And Can These Side Effects Be Predicted?
Manual Therapy 2004 (Aug); 9 (3): 151–156Hay EM, Mullis R, Lewis M, Vohora K, Main CJ, Watson P, et al.
Comparison of physical treatments versus a brief pain-management
programme for back pain in primary care: A randomised
clinical trial in physiotherapy practice.
Lancet. 2005;365: 2024–2030.
doi: 10.1016/S0140-6736(05)66696-2Bronfort G, Hondras MA, Schulz CA, Evans RL, Long CR et al (2014)
Spinal Manipulation and Home Exercise With Advice for Subacute
and Chronic Back-related Leg Pain: A Trial With Adaptive Allocation
Annals of Internal Medicine 2014 (Sep 16); 161 (6): 381—391Bronfort, G, Haas, M, Evans, R, Kawchuk, G, and Dagenais, S.
Evidence-informed Management of Chronic Low Back Pain
with Spinal Manipulation and Mobilization
Spine J. 2008 (Jan); 8 (1): 213–225Cleland JA, Glynn P, Whitman JM, Eberhart SL, MacDonald C, Childs JD.
Short-term effects of thrust versus nonthrust mobilization/
manipulation directed at the thoracic spine in patients
with neck pain: a randomized clinical trial.
Phys Ther. 2007;87: 431–440. doi: 10.2522/ptj.20060217 Available:
http://ovidsp.ovid.com/ovidweb.cgi?T=JS&PAGE=reference&D=med6&NEWS=N&AN=17341509Giles LGF, Muller R, Winter GJ.
Patient satisfaction, characteristics, radiology, and complications
associated with attending a specialized government-funded
multidisciplinary spinal pain unit.
J Manipulative Physiol Ther. 2003;26: 293–299.
doi: 10.1016/S0161-4754(03)00045-9Satpute K, Bedekar N, Hall T.
Headache symptom modification: the relevance of appropriate
manual therapy assessment and management of a patient
with features of migraine and cervicogenic headache–
a case report.
J Man Manip Ther. 2020;28: 181–188.
doi: 10.1080/10669817.2019.1662637Barrett AJ, Breen AC.
Adverse effects of spinal manipulation.
J R Soc Med. 2000;93: 258–259. Available:
http://ovidsp.ovid.com/ovidweb.cgi?T=JS&PAGE=reference&D=med4&NEWS=N&AN=10884771
doi: 10.1177/014107680009300511Meeker WC, Mootz RD, Haldeman S.
The state of chiropractic research.
Top Clin Chiropr. 2002;9: 1–13.Anderson-Peacock, E, Blouin, JS, Bryans, R et al.
Chiropractic Clinical Practice Guideline: Evidence-based
Treatment of Adult Neck Pain Not Due to Whiplash
J Canadian Chiro Assoc 2005 (Sep); 49 (3): 158–209Dagenais S, Gay RE, Tricco AC, Freeman MD, Mayer JM.
NASS Contemporary Concepts in Spine Care:
Spinal Manipulation Therapy for Acute Low Back Pain
Spine J. 2010 (Oct); 10 (10): 918–40Carlesso LC, Gross AR, Santaguida PL, Burnie S, Voth S, Sadi J.
Adverse events associated with the use of cervical manipulation
and mobilization for the treatment of neck pain in adults:
A systematic review.
Man Ther. 2010;15: 434–444.
doi: 10.1016/j.math.2010.02.006Yin P, Gao N, Wu J, Litscher G, Xu S.
Adverse Events of Massage Therapy in Pain-Related Conditions:
A Systematic Review.
Evidence-Based Complement Altern Med. 2014;2014: 1–11.
doi: 10.1155/2014/480956Coulter ID, Crawford C, Vernon H, Hurwitz EL, Khorsan R, Booth MS, et al.
Manipulation and Mobilization for Treating Chronic Nonspecific
Neck Pain: A Systematic Review and Meta-Analysis
for an Appropriateness Panel
Pain Physician. 2019 (Mar); 22 (2): E55–E70Funabashi M, Pohlman KA, Goldsworthy R, Lee A, Tibbles A, Mior S, et al.
Beliefs, perceptions and practices of chiropractors and patients
about mitigation strategies for benign adverse events
after spinal manipulation therapy.
Chiropr Man Therap. 2020;28: 46.
doi: 10.1186/s12998-020-00336-3Zhang M, Du G, Liu C, Li W, Yang J, Chen B, et al.
Efficacy and safety of Shi-style cervical manipulation therapy
for treating acute and subacute neck pain: study protocol
for a randomized controlled trial.
Trials. 2021;22: 123.
doi: 10.1186/s13063-021-05062-6Ernst E.
Prospective investigations into the safety of spinal manipulation.
J Pain Symptom Manage. 2001;21: 238–242. Available:
http://ovidsp.ovid.com/ovidweb.cgi?T=JS&PAGE=reference&D=med4&NEWS=N&AN=11239743
doi: 10.1016/s0885-3924(00)00262-1Murphy DR, Hurwitz EL, Gregory AA.
Manipulation in the Presence of Cervical Spinal Cord Compression:
A Case Series
J Manipulative Physiol Ther 2006 (Mar); 29 (3): 236—144Brantingham JW, Globe GA, Jensen ML, Cassa TK, Globe DR, Price JL, et al.
A feasibility study comparing two chiropractic protocols in
the treatment of patellofemoral pain syndrome.
J Manipulative Physiol Ther. 2009;32: 536–548.
doi: 10.1016/j.jmpt.2009.08.005JM L, Forrest L.
Withdrawal rates as a consequence of disclosure of risk
associated with manipulation of the cervical spine:
A survey.
Chiropractic & Osteopathy. 2010. p. Online access only 24 p.Bronfort G, Evans R, Anderson AV, Svendsen KH, Bracha Y, Grimm RH.
Spinal Manipulation, Medication, or Home Exercise With Advice
for Acute and Subacute Neck Pain: A Randomized Trial
Annals of Internal Medicine 2012 (Jan 3); 156 (1 Pt 1): 1–10Rajendran D, Bright P, Bettles S, Carnes D, Mullinger B.
What puts the adverse in ‘adverse events’? Patients’ perceptions
of post-treatment experiences in osteopathy–A qualitative
study using focus groups.
Man Ther. 2012;17: 305–311.
doi: 10.1016/j.math.2012.02.011Page MJ, Green S, Kramer S, Johnston R V, McBain B, Chau M, et al.
Manual therapy and exercise for adhesive capsulitis
(frozen shoulder).
Cochrane database Syst Rev. 2014; CD011275.
doi: 10.1002/14651858.CD011275Bussieres AE, Stewart G, Al-Zoubi F, Decina P, Descarreaux M, Haskett D, Hincapie C, et al.
Spinal Manipulative Therapy and Other Conservative Treatments
for Low Back Pain: A Guideline From the Canadian
Chiropractic Guideline Initiative
J Manipulative Physiol Ther. 2018 (May); 41 (4): 265–293Morris S, Booth J.
Shaping conservative spinal services with the Spine Tango Registry.
Eur Spine J. 2018;27: 543–553.
doi: 10.1007/s00586-018-5484-5Peters R, Mutsaers B, Verhagen AP, Koes BW, Pool-Goudzwaard AL.
Prospective Cohort Study of Patients With Neck Pain in a
Manual Therapy Setting: Design and Baseline Measures.
J Manipulative Physiol Ther. 2019;42: 471–479.
doi: 10.1016/j.jmpt.2019.07.001Mabry LM, Notestine JP, Moore JH, Bleakley CM, Taylor JB.
Safety Events and Privilege Utilization Rates in Advanced
Practice Physical Therapy Compared to Traditional
Primary Care: An Observational Study.
Mil Med. 2020;185: e290–e297.
doi: 10.1093/milmed/usz176Hurwitz EL:
Epidemiology: Spinal Manipulation Utilization
J Electromyogr Kinesiol. 2012 (Oct); 22 (5): 648–654Ernst E.
Adverse Effects of Spinal Manipulation: A Systematic Review
J R Soc Med. 2007 (Jul); 100 (7): 330–338Hutting N, Kerry R, Coppieters MW, Scholten-Peeters GGM.
Considerations to improve the safety of cervical
spine manual therapy.
Musculoskelet Sci Pract. 2018;33: 41–45.
doi: 10.1016/j.msksp.2017.11.003Loke YK, Golder su P, Vandenbroucke JP.
Comprehensive evaluations of the adverse effects of drugs:
Importance of appropriate study selection and data sources.
Ther Adv Drug Saf. 2011;2: 59–68.
doi: 10.1177/2042098611401129Rasmussen J.
Human error and the problem of causality in analysis of accidents.
Philos Trans R Soc Lond B Biol Sci. 1990;327.
doi: 10.1098/rstb.1990.0088Healy D.
Science, rhetoric and the causality of adverse events.
Int J Risk Saf Med. 2011;23: 149–162.
doi: 10.3233/JRS-2011-0534Rodrigues PP, Ferreira-Santos D, Silva A, Polónia J, Ribeiro-Vaz I.
Causality assessment of adverse drug reaction reports using
an expert-defined Bayesian network.
Artif Intell Med. 2018;91: 12–22.
doi: 10.1016/j.artmed.2018.07.005Bellavite P.
Causality assessment of adverse events following immunization:
The problem of multifactorial pathology.
F1000Research. 2020;9.
doi: 10.12688/f1000research.22600.1Shojania K, Duncan B, McDonald K, Wachter R, Al E.
Making health care safer: A critical analysis of patient safety practices.
Agency Healthc Res Qual. 2001.
doi: 10.1016/s1086-5802(16)30206-6Zorzela L, Mior S, Boon H, Gross A, Yager J, Carter R, et al.
Tool to assess causality of direct and indirect adverse events
associated with therapeutic interventions.
Curr Med Res Opin. 2018;34: 407–414.
doi: 10.1080/03007995.2017.1383891Doherty MJ.
Algorithms for assessing the probability of an Adverse Drug Reaction.
Respir Med CME. 2009;2: 63–67.
doi: 10.1016/j.rmedc.2009.01.004Pettker CM.
Systematic approaches to adverse events in obstetrics, Part I:
Event identification and classification.
Semin Perinatol. 2017;41: 151–155.
doi: 10.1053/j.semperi.2017.03.003Liberman JS, Liberman JS, Slagle JM, Slagle JM, Whitney G, Shotwell MS, et al.
Incidence and classification of nonroutine events during anesthesia care.
Anesthesiology. 2020; 41–52.
doi: 10.1097/ALN.0000000000003336Kaufman G.
Adverse drug reactions: classification, susceptibility and reporting.
Nurs Stand. 2016;30: 53–63.
doi: 10.7748/ns.2016.e10214Kaafarani HMA, Mavros MN, Hwabejire J, Fagenholz P, Yeh DD, Demoya M, et al.
Derivation and validation of a novel severity classification
for intraoperative adverse events.
J Am Coll Surg. 2014;218: 1120–1128.
doi: 10.1016/j.jamcollsurg.2013.12.060Albert M, Friesen F, Rowland P, Laberge S.
Problematizing assumptions about interdisciplinary research:
implications for health professions education research.
Adv Heal Sci Educ. 2020;25: 755–767.
doi: 10.1007/s10459-019-09911-7Larivičre V, Gingras Y.
Measuring interdisciplinarity.
In: Cronin B, Sugimoto C, editors. Beyond bibliometrics:
Harnessing multidimensional indicators of scholarly impact.
Cambridge, MA: MIT Press; 2014. pp. 187–200.Rozmovits L, Mior S, Boon H.
Exploring approaches to patient safety: the case
of spinal manipulation therapy.
BMC Complement Altern Med. 2016;16: 164.
doi: 10.1186/s12906-016-1149-2Rushton A, Rivett D, Carlesso L, Flynn T, Hing W, Kerry R.
International framework for examination of the cervical region
for potential of Cervical Arterial Dysfunction prior to
Orthopaedic Manual Therapy intervention.
Man Ther. 2014;19: 222–228.
doi: 10.1016/j.math.2013.11.005Stochkendahl MJ, Rezai M, Torres P, Sutton D, Tuchin P, Brown R, et al.
The chiropractic workforce: A global review.
Chiropr Man Ther. 2019;27: 1–9.
doi: 10.1186/s12998-019-0255-xHiggs J, Refshauge K, Ellis E.
Portrait of the physiotherapy profession.
J Interprof Care. 2001;15: 79–89.
doi: 10.1080/13561820020022891Osteopathic International Alliance.
Global review of osteopathic medicine and osteopathy 2020. 2020.Foo JS, Storr M, Maloney S.
Registration factors that limit international mobility of
people holding physiotherapy qualifications:
A systematic review.
Health Policy (New York). 2016;120: 665–673.
doi: 10.1016/j.healthpol.2016.04.008Hartnett DA, Milner JD, Kleinhenz DT, Kuris EO, Daniels AH.
Malpractice Litigation Involving Chiropractic Spinal Manipulation.
World Neurosurg. 2021;149: e108–e115.
doi: 10.1016/j.wneu.Cicconi M, Mangiulli T, Bolino G.
Onset of complications following cervical manipulation due
to malpractice in osteopathic treatment: a case report.
Med Sci Law. 2014;54: 230–233.
doi: 10.1177/0025802413513451Boucher P, Robidoux S.
Lumbar disc herniation and cauda equina syndrome following spinal
manipulative therapy: A review of six court decisions in Canada.
J Forensic Leg Med. 2014;22: 159–169.
doi: 10.1016/j.jflm.2013.12.026Narayan MC.
Culture’s effects on pain assessment and management.
Am J Nurs. 2010;110: 38–47; quiz 48–9.
doi: 10.1097/01.NAJ.0000370157.33223.6dAirhihenbuwa CO.
Of culture and multiverse: Renouncing
“the universal truth” in health.
J Heal Educ. 1999;30: 267–273.
doi: 10.1080/10556699.1999.10603409Dutta MJ.
Communicating About Culture and Health: Theorizing
Culture-Centered and Cultural Sensitivity Approaches.
Commun Theory. 2007;17: 304–328.
doi: 10.1111/j.1468-2885.2007.00297.xIwelunmor J, Newsome V, Airhihenbuwa CO.
Framing the impact of culture on health: A systematic review of
the PEN-3 cultural model and its application in public
health research and interventions.
Ethn Heal. 2014;19: 20–46.
doi: 10.1080/13557858.2013.857768Singhal A.
Focusing on the forest, not just the tree: cultural
strategies for combating AIDS.
Inst Strateg Mark Commun. 2003;1: 21–28. Available:
http://utminers.utep.edu/asinghal/ArticlesandChapters/singhal_forest_tree.pdf
Return to ADVERSE EVENTS
Since 5-17-2023
| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |