

Longer-term Chiropractic Care Outcomes for US Active-duty
Military Personnel with Low Back Pain: Secondary
Analysis of a Pragmatic Clinical TrialThis section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: BMC Complement Med Ther 2026 (Apr 7); 26 (1): 185 ~ FULL TEXT
OPEN ACCESS Zacariah K Shannon • Cynthia R Long • Robert D Vining • Jacob McCarey • Joan A Walter • Ian D Coulter • Christine M Goertz
Palmer College of Chiropractic,
Davenport, IA, USA.
FROM: Military.com 2019Background: Few trials have directly evaluated outcomes of adding chiropractic care to usual medical care, and prior work has been limited to short-term follow-up. The objective of this work is to address these gaps by evaluating outcomes from the addition of chiropractic care to usual medical care in active-duty U.S. military members with low back pain (LBP) over 52 weeks.
Methods: A multi-site, pragmatic clinical trial allocated 750 U.S. active-duty military personnel with LBP to usual medical care plus chiropractic care or usual medical care alone with the primary endpoint at 12 weeks. The final 154 participants enrolled in the study were asked to provide longer-term follow-up data. We used inverse probability weighting to account for missing outcome data and analyzed data using linear mixed-effects regression models over all follow-up time points. We report between-group mean differences at 12 and 52 weeks adjusted by baseline age, sex, site, pain duration, worst pain intensity, and interaction terms for site differences by group over time. Primary outcomes were disability (Roland-Morris Disability Questionnaire: RMDQ) and pain intensity (NRS). Secondary outcomes were PROMIS-29: pain interference, physical function, fatigue, sleep disturbance, and social role.
Results: A total of 144 participants provided outcome data after 12 weeks. Overall, the mean participant age was 33 years, 113 (78%) were male, 54 (38%) were non-white race, 18 (13%) were Hispanic or Latino ethnicity, and 71 (49%) had chronic LBP. At 12 weeks, moderate between-group difference in RMDQ (2.2 points, 95% CI 0.4 to 4.0) favored chiropractic care with small difference in NRS (0.6, -0.1 to 1.2). At 52 weeks, RMDQ difference was small (1.7, -0.2 to 3.7) and NRS difference was negligible (0.2, -0.5 to 1.0). Improvement in PROMIS domains varied, with many diminishing over the course of follow-up; sleep disturbance demonstrated the greatest longer-term difference in improvement at 52 weeks (3.6, 0.5 to 6.7).
Conclusions: Adding chiropractic care to usual medical care for active-duty U.S. military members with low back pain resulted in a small difference in pain-related disability and a meaningful difference in sleep disturbance but not pain intensity at 52 weeks. Differences in pain interference, physical function, and social role estimates also favored the addition of chiropractic care over the longer-term follow-up.
Trial Registration : This trial was first posted for registration on clinicaltrials.gov (NCT01692275) on 09/06/12.
Keywords: Back pain; Chiropractic; Complementary therapies; Pain management; Pragmatic clinical trial.
From the FULL TEXT Article:
Introduction
Low back pain (LBP) results in immense societal costs; it is a leading cause of global disability [1] and U.S. healthcare spending. [2] LBP is highly prevalent among people with different sociodemographic characteristics, including U.S. military members, for whom LBP has been the leading cause of medical visits for more than 10 years. [3–13] This can likely be attributed to overuse injuries and the high physical burden of military training and operations. [14]
Treatment guidelines for low back pain in U.S. military members [15] are similar to those of the general population [16], emphasizing noninvasive and nonpharmacological interventions as first-line therapies. Recommended interventions include exercise, heat, massage, spinal manipulation, other mind-body therapies, such as mindfulness-based stress reduction, tai chi, yoga, and progressive relaxation. [16] These interventions are delivered by a variety of practitioners, including medical physicians, physical therapists, and chiropractors, with guidelines recommending integrative, team-based care. [15]
Though team-based care is recommended, effects attributable to combining care from multiple providers are not well understood. Few studies have evaluated both short term and longer term effects of adding chiropractic care to usual medical care. [17] The longer-term benefit of spinal manipulation, the signature intervention of chiropractic care, compared to other recommended therapies has previously been reported to diminish by 52 weeks. [18] However, chiropractic care is typically delivered as a multimodal combination of interventions including patient education and self-management strategies, active interventions such as exercise, and passive interventions such as spinal manipulation and other manual therapies. [19–21] Evaluating longer-term outcomes of adding chiropractic care to usual medical care in a pragmatic setting is required to better inform outcome expectations for U.S. military personnel with LBP.
A pragmatic clinical trial addressed this gap by evaluating the effect of adding chiropractic care to usual medical care for U.S. military members with low back pain. Study authors found a moderate difference in improvement in pain-related disability at the end of 6-weeks of care. [22, 23] The original trial design included follow-up 12 weeks after baseline [22] predicated on anticipated combat deployment of sample participants. Because a 12-week follow-up period limits the ability to draw conclusions about longer-term effects, additional follow-up over 52 weeks was added during later stages of recruitment. The objective of this work is to evaluate and report pain-related and quality of life outcomes of chiropractic care added to usual medical care for active-duty U.S. military members with low back pain using data from a subsample of this pragmatic clinical trial.
Methods
Trial design, setting, and participants
The trial was prospectively registered (ClinicalTrials.gov identifier: NCT01692275) and the protocol was previously published. [22] The trial was a multi-site pragmatic clinical trial comparing the effects of usual medical care plus chiropractic care vs. usual medical care alone for U.S. active-duty military personnel with LBP. The trial recruited 750 active-duty military personnel, including 250 at each of 3 different military treatment facilities: Walter Reed in Bethesda, Maryland; Naval Hospital in Pensacola, Florida; and the Naval Medical Center in San Diego, California. The trial protocol included a follow-up duration of 12 weeks after enrollment, of which the primary [23] and secondary [24] results have been previously published. The final 154 of the 750 enrolled participants consented to provide follow-up data over 52 weeks after enrollment. This included only participants from the Bethesda and Pensacola sites who enrolled between October 2014 and November 2015, the end of enrollment.
The trial protocol and longer-term follow-up amendment were approved by institutional review boards at each site and the trial was overseen by an independent data and safety monitoring committee. All participants provided written informed consent. No compensation was given for participation. Medical physicians at the military treatment facilities referred patients with low back pain to the trial and performed examination and screening prior to participant enrollment. Participants were included in the trial if they were an active-duty military member reporting low back pain and aged 18–50 years. Participants were excluded for non-musculoskeletal pain, contraindication to spinal manipulation, recent spine fracture, recent spine surgery, diagnosis of post-traumatic stress disorder, or radiculopathy requiring further evaluation or referral.
Interventions
Both usual medical care and chiropractic care were delivered as usual in the military treatment facilities. Care was not dictated by trial procedures. Usual medical care included the treatment of LBP by military medical physicians and was provided to participants in both trial arms. Usual medical care interventions delivered during the trial included education and self-management strategies, medications, and referral to other providers such as physical therapists or to pain management clinics. Chiropractic care in the trial included 6 weeks of care with up to 12 visits with an on-site chiropractic clinician. A description of the component interventions and diagnoses of chiropractic care delivered to trial participants has been previously reported. [21] Common interventions of chiropractic care included treatment of the low back and surrounding area with spinal manipulation, therapeutic exercise, hot/cold packs, and electrical muscle stimulation. [21]
Outcomes
The outcomes for this secondary analysis follow the design of the trial and were specified in a pre-registered analysis plan. [25] The primary outcomes of interest are pain-related disability measured with the 0–24 Roland-Morris Disability Questionnaire (RMDQ) [26] and average low back pain intensity in the previous week measured with a 0–10 numerical rating scale (NRS). [27] The secondary outcomes of interest are the Patient-Reported Outcomes Measurement Information System (PROMIS)-29 [28] v1.0 domains of pain interference, physical function, fatigue, sleep disturbance, and social role. Previous work reported a low frequency of PROMIS-29 anxiety and depression symptoms in this trial sample which led to a skewed distribution which did not fulfill regression assumptions. [29, 30] Therefore, we did not analyze PROMIS-29 anxiety and depression outcomes for this sample. Outcomes were collected through an online data capture system which was supplemented by computer assisted telephone interviews, if needed. RMDQ and NRS were collected at baseline and weeks 2, 4, 6, 12, 26, 40, and 52 and PROMIS-29 was collected at baseline and weeks 6, 12, 26, 40, and 52. PROMIS outcome domains of physical function and social role were transformed by taking 100-(T-Score) to make a higher score indicative of worse health across all PROMIS domains.
Sample size
The trial was powered to evaluate meaningful differences in the primary outcomes of RMDQ and NRS at 3 sites, enrolling 250 participants each. Prior to data analysis, we used standard deviations and correlation coefficients from the full trial sample to conduct a power analysis for 3 outcomes to determine the effect sizes at which we would have at least 80% power to detect between-group differences at alpha = 0.05 in mixed-effects models for a 154-participant sample. RMDQ was estimated to be 2.5 points at week 12 and 2.6 points at week 52. Pain intensity was estimated to be 1.1 points at weeks 12 and 52. PROMIS pain interference estimated to be 4.2 points at week 12 and 3.9 points at week 52. Recommended effect magnitude classifications for between-group differences include 1–2 points (small) and 2–5 points (moderate) for RMDQ,16 0.5-1.0 points (small) and 1.0–2.0 points (moderate) for NRS,16 and 2–6 T-Score points for meaningful change in PROMIS measures. [31]
Randomization and allocation
Participants were randomly allocated 1:1, stratified by site, to the intervention trial arms of usual medical care plus chiropractic care or usual medical care alone using a computer-generated, adaptive, minimization algorithm. The algorithm balanced trial arms on participant characteristics of baseline age, sex, LBP duration, and pain intensity (worst in past 24 h). Allocation was concealed to participants and study personnel until after screening and enrollment in the trial.
Blinding
Blinding of participants and trial clinicians was not possible in the trial design. This analysis was not blinded.
Statistical analysis
We used SAS v9.4 (SAS Institute Inc., Cary, NC) to model each outcome in separate linear mixed-effects regression models over baseline and all follow-up time points. We followed the intent-to-treat principle analyzing participant data as assigned. Models included terms to adjust estimates by the allocation minimization covariates of baseline sex, age, pain intensity, and LBP duration and we included terms in the model for time, group and site as fixed effects and repeated measures of participants as random effects. We compared models with and without the three-way interaction term time*group*site and found this impacted some model estimates and improved model fit. Therefore, we included the three-way interaction in our models and report model estimates overall and by site. The primary endpoints of interest were 12 and 52 weeks. We report adjusted between-group mean differences and 95% confidence intervals from the models. Between-group mean differences were calculated in mixed effects models by taking UMC group – UMC + CC group, making a positive value indicative of a better outcome in the UMC + CC group. We also provide graphics of outcomes over time by site.
We performed sensitivity analyses to examine the effects of missing outcome data on results. We generated 25 datasets with multiple imputation under the missing at random assumption with chained equations using the previously described linear mixed-effects regression models. We then combined the results of the imputations and compared these to estimates of models using all observed data. For several outcomes, missing data substantially changed the effect estimates. Therefore, we chose to use a weighting procedure to create a complete dataset for statistical analysis.
We used an inverse probability weighting method for missing longitudinal data. [32–34] We first modelled the probability of missing data for each outcome using logistic regression and a stepwise covariate selection process with a conservative alpha = 0.25 for entrance and removal. We included the model covariates of time, group, site, sex, age, worst pain intensity, and LBP duration and used the stepwise selection process to assess the baseline covariates of race, ethnicity, RMDQ, NRS, and PROMIS outcome domains. These baseline characteristic variables were chosen to be assessed based on expectation of relatedness to missingness. We used linear mixed-effects regression models weighted by the inverse of the probability of missingness to generate predicted values for missing outcomes. Missing outcomes were replaced with these predicted values to generate a dataset consisting of complete data for all outcomes at all time points.
Results
Participants and treatment visits
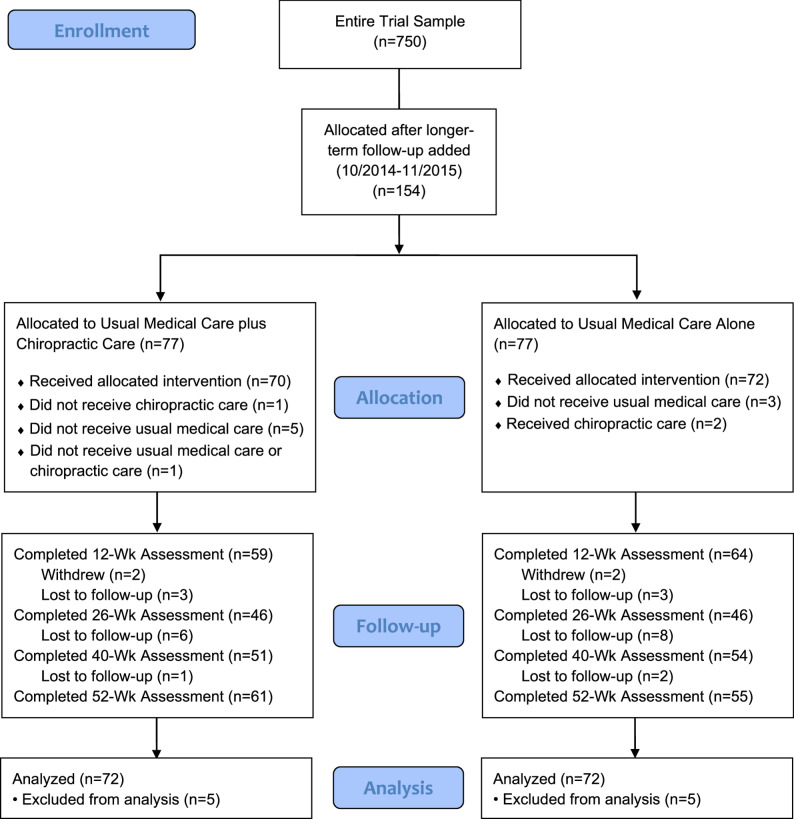
Figure 1 A flow diagram for the trial is shown in Figure 1. Of the 750 total participants, 154 enrolled after the longer-term follow-up was added to the protocol in 9/2014. Missing data varied by follow-up time point. There was no missing baseline data and there were more missing data at later follow-up time points than at 6 and 12 weeks. At 12 weeks or later, non-missing outcome data for RMDQ and NRS ranged from 64 to 76% and from 42 to 86%. for PROMIS outcomes. In each trial arm, 2 participants withdrew and 3 were lost to follow-up before the 12-week follow-up and were excluded from this analysis. The result was an analysis of data from 144 participants.

Table 1 Table 1 shows baseline participant data overall and by site for the 144 participants included in this analysis. Fifty-one of the participants were enrolled at the Pensacola site and 93 at Bethesda. The mean participant age was 33 years, 113 (78%) were male, 54 (38%) were non-white race, 18 (13%) were Hispanic or Latino ethnicity, and 71 (49%) had chronic LBP. However, baseline characteristics varied by site, with participants at the Pensacola site were younger with a higher percentage of male sex and white race. Participants reported moderate to high LBP-related disability, high pain interference, but less anxiety and depression symptoms than the general population (mean T-Scores < 50) and fatigue symptoms approximately equivalent to the general population (mean T-Score ≈ 50). Baseline measures were similar for most variables between trial arms and were consistent with baseline characteristics reported for the full trial sample. [23]
Outcomes
Table 2
Figs 2-8 Table 2 displays the between-group mean differences and 95% confidence intervals for each outcome by site and overall, at 12 and 52 weeks. Figures 2, 3, 4, 5, 6, 7 and 8 show the estimated means at each outcome by site across all time points. Overall, between-group mean difference in RMDQ favored the UMC + CC group at weeks 12 and 52. The overall difference in NRS at week 12 was small in magnitude and diminished to a negligible difference at week 52. Overall, 12-week mean differences were noted for PROMIS pain interference (4.0 points, 95% CI 1.6 to 6.5) and social role (3.8 points, 95% CI 0.9 to 6.7). Compared to 12 weeks, mean differences at 52 weeks were smaller for pain interference (2.3 points, 95% CI -0.7 to 5.2) and social role (2.1 points, 95% CI -0.5 to 4.7), but were larger for physical function (2.1 points, 95% CI -0.8 to 4.9) and sleep disturbance (3.6 points, 95% CI 0.5 to 6.7).
Discussion
We found that adding chiropractic care to usual medical care resulted in moderate improvement in pain-related disability and small improvement in pain intensity in the short-term. These findings are consistent with those reported in the original analysis of 6 and 12 week outcomes from the entire 750 participant sample. [23] At 52 weeks, however, we found a small difference in pain-related disability and negligible difference in pain intensity. For PROMIS domains, differences favoring the addition of chiropractic care for pain interference and social role reduced over the course of longer-term follow-up. The greatest longer-term difference in PROMIS-29 domains was for sleep disturbance, which showed a meaningful difference at 52 weeks. Previous work from this trial also reported short-term improvement in sleep disturbance. [24] Our finding that this benefit was sustained at 52 weeks is potentially important given the established relationship between sleep quality and musculoskeletal pain in the military [35] and beyond. [36–41] Further study of the effect of chiropractic care on sleep quality is needed to determine if our findings are reproducible.
Active-duty military enrolled in the trial reported very few mental health symptoms at baseline. The mean PROMIS anxiety and depression T-Scores were better than the general population average as indicated by T-Scores < 50. While it is possible that a young and physically active population, characteristic of U.S. active-duty military, may experience less mental health symptoms, it is widely recognized that mental health symptoms are underreported by U.S. military members. [42–44] Future study of populations reporting mental health symptoms is needed to better understand longer-term effects of chiropractic care on mental health.
Chiropractic care delivered to trial participants included a number of nonpharmacological interventions, most commonly spinal manipulation and therapeutic exercise. [21] Compared to usual care, a combination of patient reassurance, recommendations on exercise and avoiding passive treatments, over the counter pain medication, and spinal manipulation delivered by chiropractors has led to greater improvement in functioning, but not pain. [45] In a more direct comparison to the population studied in our trial, previous work has shown that U.S. military members with LBP receiving early treatment with nonpharmacological approaches, including chiropractic care, achieve greater improvement in function one year after initiation of care compared to treatment without early nonpharmacological approaches. [46]
Work comparing spinal manipulation to back school and individualized physiotherapy in an outpatient rehabilitation setting reported greater improvement in function and pain at 52 weeks with spinal manipulation, but with a substantially greater number of visits. [47] Interventions requiring a greater number of clinic visits may pose an implementation challenge for military treatment facilities, where U.S. military members have limited access to follow-up care for LBP. [48] As a consequence of limited access, care for U.S. military members with LBP is largely delivered outside of military treatment facilities through coverage provided by TRICARE. However, TRICARE does not cover chiropractic care. [49] A strength of our pragmatic trial design is that it evaluated outcomes with the addition of chiropractic care to usual medical care in military treatment facilities, the current mode through which U.S. military personnel receive covered chiropractic care.
This study provides additional evidence that care delivered by chiropractors is an effective approach for producing small to moderate effects on outcomes in the treatment of LBP. Results further suggest that active-duty military personnel receiving chiropractic care in military treatment facilities have improved quality of life outcomes in the short and longer term. Barriers to implementing these findings include a limited number of chiropractors employed in military treatment facilities and a lack of TRICARE coverage for chiropractic care in the private sector. Health policy changes are necessary to address barriers to chiropractic care access for delivery at scale.
Limitations
This secondary analysis was not powered to detect small differences that are typical of nonpharmacological interventions for pain. The power calculation conducted prior to our analysis suggested the sample would provide power to detect moderate between-group differences for the outcomes. Our effect estimates for the 52-week outcomes of pain interference, physical function, and social role were just above 2 T-Score points, the lower threshold of suggested meaningful difference for PROMIS measures. [31]
There was substantial missing outcome data in the longer-term follow-up due to this trial being conducted in a mobile active-duty military population. Rather than reporting only complete cases, we followed a process of assessing the effects of missing data on effect estimates. To address bias associated with missing outcome data, we used a conservative approach in selecting covariates and replacing missing outcome values before analyzing a complete dataset. [50]
Health care utilization during the longer-term follow-up was not collected, limiting the ability to assess differences in care seeking over the longer-term. There was a possibility of cross-contamination over the course of follow-up, whereby participants could have received care that was beyond the scope of the intervention assigned in the trial. Possible contributors to site differences include structural barriers, e.g. access to care or resource availability constraining the number of healthcare visits, varying clinician approach, and/or varying patient characteristics, among others. Future research aimed at differentiating these factors could be used to inform a more optimal approach to chiropractic care.
Conclusions
Adding chiropractic care to usual medical care for active-duty U.S. military members with low back pain resulted in a small difference in pain-related disability and a meaningful difference in sleep disturbance but not pain intensity at 52 weeks. Differences in pain interference, physical function, and social role estimates also favored the addition of chiropractic care over the longer-term follow-up.
Authors’ contributions
ZKS wrote the main manuscript text and prepared the figures and tables.
ZKS, CRL, and JM contributed to the data analysis.
CRL, RDV, JAW, IDC, and CMG contributed to the study concept development and design.
All authors reviewed the manuscript and contributed significantly to revision of the manuscript.
Funding
This clinical trial was supported by grant W81XWH-11-2-0107 from the Congressionally Directed Medical Research Program, US Army, US Department of Defense.
Zacariah Shannon was supported during this work by National Institutes of Health/National Center for Complementary and Integrative Health Loan Repayment Grant: L30AT013015.
The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health nor reflect the position or policy of the U.S. Department of Defense or the United States Government.
Competing interests
The authors declare no competing interests.
References:
GBD 2017 Disease and Injury Incidence and Prevalence Collaborators.
Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017.
Lancet Lond Engl. 2018;392(10159):1789–858.
10.1016/S0140-6736(18)32279-7.Dieleman JL, Cao J, Chapin A, et al.
US Health Care Spending by Payer
and Health Condition, 1996-2016
JAMA 2020 (Mar 3); 323 (9): 863–884Yuan X, Pav V, Colahan C, et al.
Active duty service members newly presenting with low back pain in fiscal year 2017: health care utilization, access to care, and private sector costs over 2-year follow-up.
Mil Med. 2023;188(7–8):2387–96.Armed Forces Health Surveillance Center (AFHSC).
Absolute and relative morbidity burdens attributable to various illnesses and injuries, U.S. Armed Forces, 2014.
MSMR. 2015;22(4):5–10.Armed Forces Health Surveillance Branch.
Absolute and relative morbidity burdens attributable to various illnesses and injuries, active component, U.S. Armed Forces, 2015.
MSMR. 2016;23(4):2–7.Armed Forces Health Surveillance Branch.
Absolute and relative morbidity burdens attributable to various illnesses and injuries, active component, U.S. Armed Forces, 2016.
MSMR. 2017;24(4):2–8Armed Forces Health Surveillance Branch.
Absolute and relative morbidity burdens attributable to various illnesses and injuries, active component, U.S. Armed Forces, 2017.
MSMR. 2018;25(5):2–9Absolute. relative morbidity burdens attributable to various illnesses and injuries, active component, U.S. Armed Forces, 2018.
MSMR. 2019;26(5):2–10Absolute. relative morbidity burdens attributable to various illnesses and injuries, active component, U.S. Armed Forces, 2019.
MSMR. 2020;27(5):2–9.Absolute and relative morbidity burdens attributable to various illnesses and injuries, active component, U.S. Armed Forces, 2020.
MSMR. 2021;28(5):2–9Armed Forces Health Surveillance Division.
Absolute and relative morbidity burdens attributable to various illnesses and injuries, active component, U.S. Armed Forces, 2021.
MSMR. 2022;29(6):2–9.Armed Forces Health Surveillance Division.
Absolute and Relative Morbidity Burdens Attributable to Various Illnesses and Injuries Among Active Component Members, U.S. Armed Forces, 2022.
MSMR. 2023;30(6):3–11Armed Forces Health Surveillance Division.
Absolute and relative morbidity burdens attributable to various illnesses and injuries among active component members of the U.S. Armed Forces, 2023.
MSMR. 2024;31(6):2–10Hauret KG, Jones BH, Bullock SH, Canham-Chervak M.
Musculoskeletal Injuries: Description of an Under-Recognized Injury Problem Among Military Personnel.
Am J Prev Med. 2010;38(1, Supplement):S61–70.
10.1016/j.amepre.2009.10.021.Pangarkar SS, Kang DG, Sandbrink F, et al.
VA/DoD Clinical Practice Guideline: Diagnosis and Treatment of Low Back Pain.
J Gen Intern Med. 2019;34(11):2620–9.
10.1007/s11606-019-05086-4Qaseem A, Wilt TJ, McLean RM, Forciea MA,
Noninvasive Treatments for Acute, Subacute, and Chronic
Low Back Pain: A Clinical Practice Guideline From
the American College of Physicians
Annals of Internal Medicine 2017 (Apr 4); 166 (7): 514–530Blanchette MA, Stochkendahl MJ, Borges Da Silva R, Boruff J.
Effectiveness and Economic Evaluation of Chiropractic
Care for the Treatment of Low Back Pain:
A Systematic Review of Pragmatic Studies
PLoS One. 2016 (Aug 3); 11 (8): e0160037Rubinstein SM, de Zoete A, van Middelkoop M
Benefits and Harms of Spinal Manipulative Therapy for the
Treatment of Chronic Low Back Pain: Systematic Review
and Meta-analysis of Randomised Controlled Trials
British Medical Journal 2019 (Mar 13); 364: 1689Vining RD, Shannon ZK, Salsbury SA, Corber L.
Development of a Clinical Decision Aid for Chiropractic
Management of Common Conditions Causing Low Back
Pain in Veterans: Results of a Consensus Process
J Manipulative Physiol Ther. 2019 (Nov); 42 (9): 677–693National Board of Chiropractic Examiners.
Practice Analysis of Chiropractic 2020
Ziegler AML, Shannon Z, Long CR, et al.
Chiropractic Services and Diagnoses for Low Back
Pain in 3 U.S. Department of Defense Military
Treatment Facilities: A Secondary Analysis
of a Pragmatic Clinical Trial
J Manipulative Physiol Ther 2021 (Nov); 44 (9): 690–698Goertz CM, Long CR, Vining RD, et al.
Assessment of Chiropractic Treatment for Active Duty,
U.S. Military Personnel With Low Back Pain:
Study Protocol for a Randomized
Controlled Trial
Trials. 2016 (Feb 9); 17: 70Goertz CM, Long CR, Vining RD, Pohlman KA, Walter J, Coulter I.
Effect of Usual Medical Care Plus Chiropractic Care
vs Usual Medical Care Alone on Pain and Disability
Among US Service Members With Low Back Pain
JAMA Network Open. 2018 (May 18); 1 (1): e180105Hays RD, Shannon ZK, Long CR, et al.
Health-related Quality of Life Among United States Service
Members with Low Back Pain Receiving Usual Care plus
Chiropractic Care plus Usual Care vs Usual Care Alone:
Secondary Outcomes of a Pragmatic Clinical Trial
Pain Medicine 2022 (Aug 31); 23 (9): 1550–1559Shannon Z.
Longer-term outcomes and mediators of chiropractic care for active-duty military with low back pain.
Published online Oct. 2024;1. 10.17605/OSF.IO/W5YB8.Roland M, Morris R.
A study of the natural history of back pain. Part I: development of a reliable and sensitive measure of disability in low-back pain.
Spine. 1983;8(2):141–4.
10.1097/00007632-198303000-00004.Childs JD, Piva SR, Fritz JM.
Responsiveness of the numeric pain rating scale in patients with low back pain.
Spine. 2005;30(11):1331–4.
10.1097/01.brs.0000164099.92112.29.PROMIS Health Organization and PROMIS Cooperative Group.
Patient-Reported Outcomes Measurement Information System (PROMIS). 2023.
https://commonfund.nih.gov/promis/index
Accessed December 18.Shannon ZK, Long CR, Chrischilles EA, et al.
Effect of Chiropractic Care on Low Back Pain
for Active-duty Military Members: Mediation
Through Biopsychosocial Factors
PLoS One 2024 (Oct 1); 19 (10): e0310642Shannon ZK, Long CR, Chrischilles E, et al.
Secondary Causal Mediation Analysis of a Pragmatic Clinical
Trial to Evaluate the Effect of Chiropractic Care for US
Active-duty Military on Biopsychosocial Outcomes
Occurring Through Effects on Low Back Pain
Interference and Intensity
BMJ Open 2024 (Nov 19); 14 (11): e083509689Terwee CB, Peipert JD, Chapman R, et al.
Minimal important change (MIC): a conceptual clarification and systematic review of MIC estimates of PROMIS measures.
Qual Life Res. 2021;30(10):2729–54.
10.1007/s11136-021-02925-ySeaman SR, White IR.
Review of inverse probability weighting for dealing with missing data.
Stat Methods Med Res. 2013;22(3):278–95.
10.1177/0962280210395740Little RJ, Carpenter JR, Lee KJ.
A Comparison of Three Popular Methods for Handling Missing Data: Complete-Case Analysis, Inverse Probability Weighting, and Multiple Imputation.
Sociol Methods Res. 2024;53(3):1105–35.
10.1177/00491241221113873.Seaman SR, Vansteelandt S.
Introduction to Double Robust Methods for Incomplete Data.
Stat Sci Rev J Inst Math Stat. 2018;33(2):184–97.
10.1214/18-STS647.Rhon DI, O’Hagan E, Mysliwiec V, Lentz TA.
Does Disordered Sleep Moderate the Relationship Between Pain, Disability and Downstream Health Care Utilization in Patients With Low Back Pain? A Longitudinal Cohort From the US Military Health System.
Spine. 2019;44(21):1481–91.
10.1097/BRS.0000000000003114.Alsaadi SM, McAuley JH, Hush JM, et al.
The Bidirectional Relationship Between Pain Intensity and Sleep Disturbance/Quality in Patients With Low Back Pain.
Clin J Pain. 2014;30(9):755–65.
10.1097/AJP.0000000000000055.Finan PH, Goodin BR, Smith MT.
The association of sleep and pain: an update and a path forward.
J Pain. 2013;14(12):1539–52.
10.1016/j.jpain.2013.08.007.Generaal E, Vogelzangs N, Penninx BWJH, Dekker J,
Insomnia, Sleep Duration, Depressive Symptoms, and the Onset of Chronic Multisite Musculoskeletal Pain.
Sleep. 2017;40(1).
10.1093/sleep/zsw030Pan F, Tian J, Cicuttini F, Jones G.
Sleep Disturbance and Its Association with Pain Severity and Multisite Pain: A Prospective 10.7-Year Study.
Pain Ther. 2020;9(2):751–63.
10.1007/s40122-020-00208-xAfolalu EF, Ramlee F, Tang NKY.
Effects of sleep changes on pain-related health outcomes in the general population: A systematic review of longitudinal studies with exploratory meta-analysis.
Sleep Med Rev. 2018;39:82–97.
10.1016/j.smrv.2017.08.001Aili K, Nyman T, Svartengren M, Hillert L.
Sleep as a predictive factor for the onset and resolution of multi-site pain: a 5-year prospective study.
Eur J Pain Lond Engl. 2015;19(3):341–9.
10.1002/ejp.552.Greene-Shortridge TM, Britt TW, Castro CA.
The stigma of mental health problems in the military.
Mil Med. 2007;172(2):157–61.
10.7205/milmed.172.2.157.Schreiber M, McEnany GP,
Stigma. American military personnel and mental health care: challenges from Iraq and Afghanistan.
J Ment Health Abingdon Engl. 2015;24(1):54–9.
10.3109/09638237.2014.971147.Clement S, Schauman O, Graham T, et al.
What is the impact of mental health-related stigma on help-seeking? A systematic review of quantitative and qualitative studies.
Psychol Med. 2015;45(1):11–27.
10.1017/S0033291714000129.Bishop PB, Quon JA, Fisher CG, Dvorak MFS.
The Chiropractic Hospital-based Interventions Research Outcomes (CHIRO) Study: a randomized controlled trial on the effectiveness of clinical practice guidelines in the medical and chiropractic management of patients with acute mechanical low back pain.
Spine J. 2010;10(12):1055–64.
10.1016/j.spinee.2010.08.019.Larson MJ, Adams RS, Ritter GA, et al.
Associations of Early Treatments for Low-Back Pain with Military Readiness Outcomes.
J Altern Complement Med. 2018;24(7):666–76.
10.1089/acm.2017.0290.Cecchi F, Molino-Lova R, Chiti M, et al.
Spinal Manipulation Compared with Back School
and with Individually Delivered Physiotherapy
for the Treatment of Chronic Low Back Pain:
A Randomized Trial with One-year Follow-up
Clinical Rehabilitation 2010 (Jan); 24 (1): 26–36Taylor J, Travaglini L, O’Connell M, et al.
Inequities time-to-follow-up care and administrative action after low back pain diagnosis in active duty service members.
Pain Published online Febr. 2025;28.
10.1097/j.pain.0000000000003559.Yuan X, Pav V, Colahan C, et al
Active duty service members newly presenting with low back pain in fiscal year 2017: health care utilization, access to care, and private sector costs over 2-year follow-up.
Mil Med. 2023;188(7–8):e2387–e96.
10.1093/milmed/usac363.Schulz KF, Grimes DA.
Sample size slippages in randomised trials: exclusions and the lost and wayward.
Lancet Lond Engl. 2002;359(9308):781–5.
Return to LOW BACK PAIN
Return to CHIROPRACTIC CARE FOR VETERANS
Since 6-06-2026


| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |