

The Association Between Chiropractic Integration in an Ontario
Community Health Centre and Continued Prescription Opioid
Use for Chronic Non-cancer Spinal Pain: A Sequential
Explanatory Mixed Methods StudyThis section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: BMC Health Serv Res 2022 (Nov 3); 22 (1): 1313 ~ FULL TEXT
OPEN ACCESS Peter C Emary • Amy L Brown • Mark Oremus • Lawrence Mbuagbaw • Douglas F Cameron • Jenna DiDonato • Jason W Busse
Faculty of Health Sciences,
Ontario Tech University.
Background: Emerging evidence suggests that access to chiropractic care may reduce the likelihood of initiating an opioid prescription for spinal pain; however, the impact of chiropractic care for patients already prescribed opioids is uncertain. We undertook a sequential explanatory mixed methods study to evaluate the association between initiating chiropractic care and continued opioid use among adult patients attending an Ontario community health centre (CHC) and receiving opioid therapy for chronic non-cancer spinal pain.
Methods: We conducted a retrospective cohort study of 210 patient records between January 1, 2014 and December 31, 2020. We used generalized estimating equations, adjusted for patient demographics, co-morbidities, visit frequency, and calendar year, to evaluate the association between receipt versus non-receipt of chiropractic services and continued opioid use (e.g., unique opioid fills, number of refills, and dosages) up to one year following the index chiropractic visit. We also completed follow-up interviews with 14 patients and nine general practitioners from the CHC and integrated these data with our quantitative findings.
Results: Over 12-month follow-up, there were lower rates of opioid fills (incidence rate ratio [IRR] = 0.66; 95% confidence interval [CI], 0.52-0.83) and refills (IRR = 0.27; 95% CI, 0.17-0.42) among chiropractic recipients (n = 49) versus non-recipients (n = 161). Although patients who did and did not receive chiropractic care began the study with the same dose of opioids, recipients were less likely to be prescribed higher-dose opioids (i.e., ? 50 mg morphine equivalents daily) compared to non-recipients at three months (odds ratio [OR] = 0.14; 95% CI, 0.04-0.47), six months (OR = 0.14; 95% CI, 0.05-0.40), nine months (OR = 0.19; 95% CI, 0.07-0.57), and 12 months (OR = 0.22; 95% CI, 0.08-0.62). Interviews suggested that patient self-efficacy, limited effectiveness of opioids for chronic pain, stigma regarding use of opioids, and access to chiropractic treatment were important influencing factors.
Conclusion: We found that continued prescription opioid use among patients with chronic non-cancer spinal pain who received chiropractic care was lower than in patients who did not receive chiropractic care. Four themes emerged in our qualitative interviews to help provide a richer understanding of this association. Randomized controlled trials are needed to establish the effect of chiropractic care on opioid use for chronic spinal pain.
Keywords: Chiropractic; Community Health Centres; Health Services Research; Mixed methods; Opioids.
From the FULL TEXT Article:
Background
Chronic non-cancer pain affecting the spine or other musculoskeletal tissues is a prevalent and global health problem associated with considerable socioeconomic burden. Worldwide, approximately one in five people live with chronic non-cancer pain [1–4], with seniors, women, military veterans, indigenous populations, rural inhabitants, those with lower formal education, and individuals reporting low socioeconomic status being most affected. [5–7] In Canada, the annual economic cost of chronic non-cancer pain due to medical expenditures and lost productivity was estimated between $38 and $40 billion in 2019, and this cost is expected to rise by more than 36% by the year 2030. [8] The annual cost of chronic non-cancer pain in the United States (US) was previously estimated to be between $560 and $635 billion. [9] Opioids are commonly prescribed to patients to relieve chronic non-cancer pain, particularly in North America [10]; however, opioids provide only modest benefits [11] and are associated with important dose-dependent harms, including overdose and death. [12–15] Accordingly, governments, policy makers, and insurers have been called upon to improve support for non-opioid approaches to managing chronic non-cancer pain, particularly in vulnerable and marginalized populations. [16]
Emerging evidence suggests that early access to chiropractic treatment is associated with lower initiation of opioid prescribing among patients with non-cancer spinal pain. [17–21] A 2020 systematic review and meta-analysis of six cohort studies found that patients with acute or chronic non-cancer spinal pain who received chiropractic services early in their complaint were 64% less likely than non-chiropractic users to be prescribed opioids (pooled odds ratio [OR] = 0.36; 95% confidence interval [CI], 0.30 to 0.43). [17] A subsequent observational study of 216,504 opioid-naive patients with new-onset low back pain who received initial treatment from chiropractors versus primary care physicians had 90% lower odds of short-term opioid use (adjusted OR = 0.10; 95% CI, 0.09 to 0.10) and 78% lower odds of long-term opioid use (adjusted OR = 0.22; 95% CI, 0.18 to 0.26). [18, 19] Similar findings have been reported by two other recent observational studies [20, 21]; however, the association between receipt of chiropractic services and continued opioid use in patients with existing opioid prescriptions is uncertain. [22–24] Moreover, previously published studies on the topic of chiropractic care and opioid prescribing have lacked in-depth, contextual understanding because they have been exclusively quantitative in nature. [17–24]
Editorial Comment: An Odds Ratio (OR) of 0.10 indicates a strong negative association, meaning the odds of an outcome occurring are 90% lower in the treatment or exposed group, compared to the control group. To help address these knowledge gaps, we conducted a mixed methods study to evaluate the association between initiating chiropractic care and continued opioid use among adult patients with chronic non-cancer spinal pain attending an Ontario community health centre (CHC). [25, 26]
We hypothesized that younger age, male sex, health-related co-morbidities, depressive symptoms, poor health behaviours (e.g., smoking), a higher frequency of healthcare provider visits, and earlier years of our 7-year study timeframe would be positively associated with opioid use. We also hypothesized that chiropractic care would be inversely associated with opioid use. [25]
Methods
Ethical considerations
Our study was approved by the Hamilton Integrated Research Ethics Board at McMaster University (project number 2021–10930). Approval to conduct this study was also obtained from the Chief Executive Officer at the Langs CHC. [26] All methods were carried out in accordance with the relevant guidelines and regulations and the Declaration of Helsinki.
Study design
We used a sequential explanatory mixed methods design. [27] In the quantitative phase, we obtained data via chart review [28] of electronic medical records (EMRs) of both recipients and non-recipients of chiropractic services with at least one prescribed opioid for the treatment of a chronic non-cancer spinal pain-related diagnosis at the Langs CHC. [26]

Figure 1 In the qualitative phase, we conducted one-on-one interviews with patients and general practitioners (GPs) to explore perceptions of chiropractic integration on opioid prescribing. Complementarity [29] was our rationale for using a mixed methods approach, that is, the results from the qualitative phase of our study were used to help clarify and explain our quantitative findings. See Figure 1 for a diagram outlining our study procedures.
We followed the STROBE statement [30], the COREQ criteria [31], and the Good Reporting of A Mixed Methods Study (GRAMMS) guidelines [32, 33] for our study (Additional file 1).
Setting
The Langs CHC is located in Cambridge, Ontario, Canada [25, 26], a medium-sized urban municipality (population: ~130,000) located 82 km southwest of Toronto. This Centre provides healthcare services to communities and vulnerable populations with high unemployment rates, multiple co-morbidities, and musculoskeletal disorders that are commonly managed with prescription opioids. [25, 26] Because chiropractic services are not publicly funded in Canada, these populations have traditionally faced barriers to accessing chiropractic care. [23, 34–40] However, since January 1, 2014 [34] a partially subsidized chiropractic spine pain program that operates on two half days per week has been offered to patients at the Centre. To be eligible to receive these services, patients have to be referred into the program by their GP.
The Centre also employs a team of medical doctors, nurse practitioners, registered nurses, dieticians, social workers, community health workers, and a physiotherapist. For more complete details of the CHC’s chiropractic spine pain program, our conceptual framework, and a list of diagnostic codes used for defining our study sample, we refer readers to our study protocol. [25]
Quantitative samplingParticipants and data sources
We included records for all adult patients (aged ≥ 18 years) who received one or more prescriptions for opioids dispensed over a minimum period of three consecutive months, and who attended two or more appointments relating to a diagnosis of chronic spine (i.e., back or neck) pain at the Langs CHC between January 1, 2014, and December 31, 2020. The start date for quantitative sampling was January 1, 2014, which was the inaugural date of the Langs CHC’s chiropractic spine pain program. [34]
Patients receiving treatment for opioid use disorder (e.g., methadone, naloxone) prior to their index visit, as well as those with spinal neoplasms or other contraindications to chiropractic treatment (i.e., fractures, infections, inflammatory arthritis, or cauda equina syndrome), were excluded from our cohort. As we were interested in patients receiving long-term opioid therapy [13], we excluded individuals who had been prescribed opioids for < 90 days at their index visit, or who did not receive any opioid fills or refills after their index visit.
We linked EMR records of all patients in our study to medical drug claims data at the Institute for Clinical Evaluative Sciences (ICES) (https://www.ices.on.ca) with their Ontario health card number. ICES is an independent, non-profit research institute whose legal status under Ontario’s health information privacy law allows for the collection and analysis of healthcare and demographic data, without consent, for health system evaluation and improvement. Patients whose health card number was incorrectly recorded in their EMR were excluded.
Quantitative data collection
Variables Opioid prescription data were obtained from the Narcotics Monitoring System database by an independent research scientist at ICES, including the number of prescribed opioid fills, the number of prescribed opioid refills (measured in 30-day equivalents), and the prescribed opioid dosage. These outcomes were measured for up to 12 months from the date of first opioid prescription following a patient’s index visit for chronic non-cancer spinal pain. To maintain temporality, the index visit for patients who received chiropractic care was their first chiropractic visit. Other variables that were extracted from the EMR included socio-demographics (age and sex), general health (smoking status and body mass index), co-morbidities (depression, anxiety, fibromyalgia, diabetes, and cardiovascular disease), and the total number of healthcare (i.e., GP or chiropractic) visits. These variables have been shown to be associated with opioid use. [22, 41–48] To increase the reliability of data extraction [28], an independent information technology specialist, who was blinded to the research questions, extracted all patient data directly from the Langs EMR database. [25]
Quantitative data analysis
Statistical methods Baseline characteristics were compared between the exposed (receipt of chiropractic care) and non-exposed groups using the chi-squared test for categorical variables (or Fisher’s exact test if there was a cell frequency of < 5) and the Mann-Whitney U test for skewed continuous variables. We used generalized estimating equations (GEEs) to explore the association between exposure to chiropractic care and opioid prescribing. [49, 50]
To account for potential data clustering within-subjects or between medical or chiropractic practitioners, we used a robust variance estimator to compute the standard errors for our coefficient estimates. We also conducted sensitivity analyses with different working correlation structures, including independent, autoregressive, and unstructured matrices. [49, 50] The specified link function in our GEE models was based on the data distribution (e.g., log-linear for data fitting a Poisson distribution, binomial for binary data).
We used GEEs with a Poisson distribution when the outcomes were counts (i.e., total number of unique opioid fills and subsequent refills over the entire course of follow-up, tabulated at the end of follow-up). We estimated incidence rate ratios (IRRs) for differences between the chiropractic and non-chiropractic groups using Poisson log-linear GEEs and reported the associated 95% CIs and p-values.
We used GEEs with a binomial distribution when the outcome was opioid dosage. We assessed opioid dosages at 90-day intervals, dichotomized into higher (≥ 50 mg) morphine equivalents daily (MED) or lower (< 50 mg) MED [11] and compared these between the chiropractic and non-chiropractic groups from baseline to 12-month follow-up. We originally planned to dichotomize opioid dose using a different threshold (≥ 90 mg versus < 90 mg MED) [25], but we modified our approach to reflect the central tendency of MED in our patient sample. We estimated between-group differences for dosage using a binary logistic GEE and reported these with ORs, 95% CIs, and p-values. To calculate the MED for each prescribed opioid, we multiplied the quantity × the milligrams per unit dispensed × drug-specific conversion factors (Additional file 2). [11, 13]
Quantitative variables and study size
For each outcome of interest, we built univariable and multivariable models to estimate the crude and adjusted associations, respectively, between patients that did or did not receive chiropractic care (1 = received; 0 = did not receive) and opioid use. We grouped covariates into blocks (e.g., socio-demographic, health-related, depressive symptoms, health behaviours, and healthcare visits) and these were sequentially entered into our models, with time (i.e., calendar year) as an additional covariate and chiropractic/non-chiropractic care as the main exposure variable. To guard against over-fitting of our regression models [51], we set a minimum threshold of 10 events per category for each independent variable (i.e., minimum sample of 150 patient records) to ensure that each variable had sufficient discriminant power to detect an association with opioid use, if an association existed.
We assessed model fit using the quasi-likelihood under the independence model criterion (QIC). [50, 52] Correlation structures with the lowest QIC scores (closest to zero) were judged as the best model fit for the data. We also explored variance inflation factors (VIFs) to assess collinearity between independent variables. If multicollinearity was detected between two or more variables (i.e., VIFs ≥ 5) [53], we compared regression models, each separately containing one of the collinear variables, to one another and selected the model containing the variable that produced the lowest Akaike information criterion (AIC) value. The two-sided statistical significance level (Inline graphic) for all quantitative analyses was 5%, and all data and comparative analyses were performed using SPSS v28.0.1.0 (IBM SPSS Statistics).
Qualitative sampling
For the qualitative phase of our study, we used stratified purposive sampling to select a sub-sample of chiropractic and non-chiropractic patients, whose charts we examined in the quantitative phase, to participate in one-on-one interviews. [54] This was the first stage of integration between our quantitative and qualitative study phases. [55] We also recruited a purposive sample of GPs from the Langs CHC. The lead author (PCE) conducted recruitment via telephone or e-mail using participant contact information provided by the Langs CHC administration. We offered gift cards ($10 for GPs, $30 for patients) as incentives for participation.
We used maximum variation [54] in choosing participants, based on age, sex, and the number of years attending the CHC (for patients) or years in practice (for GPs), to encourage a range of sociodemographic characteristics and perspectives. We also collected patients’ primary spine pain complaint and current opioid dose. We aimed to interview a minimum of 12–20 patients and 6–10 GPs [54], with interviews continuing until saturation; the point at which no new information was obtained from participants in the GP, chiropractic, and non-chiropractic groups. [56] We used fundamental qualitative description [56, 57] as our methodological orientation to underpin the qualitative phase of our study.Qualitative data collection
The lead author (PCE), a health research methodologist with expertise in mixed methods and qualitative research, conducted one-on-one (individual) semi-structured interviews with participants. Interviews were conducted either virtually (n = 3) using the Zoom videoconferencing application (Zoom Video Communications, Inc.) or in-person (n = 20), based on participant preference. We promoted confidentiality by conducting the interviews in a private office separate from the medical clinic at the Langs CHC. We obtained informed consent from participants before the start of each interview. Five members of our research team (PCE, ALB, MO, LM, JWB) developed the patient and GP interview guides (see Additional files 3 and 4, respectively) based on relevant literature [17–24, 27] and our quantitative findings. Three of the five members (PCE, ALB, JWB) also have content expertise in the subject area of our study.
We audio recorded virtual interviews using Zoom’s built-in recording feature and in-person interviews using MacIntosh recording software (Audio Recorder v1.3, FIPLAB Ltd.). The lead author (PCE) also took field notes after each interview to document other observations and emergent themes. To promote trustworthiness in our qualitative data, we employed member-checking [27] by sending the raw transcripts and a summary of our results to participants for feedback or correction. We also kept an audit trail of our qualitative data collection and analysis procedures. [56] A summary of our investigator reflexivity is provided in Additional file 5.
Qualitative data analysis
We transferred all interview audio recordings into the software program, MAXQDA (http://www.maxqda.com), and the lead author (PCE) transcribed the audio recordings verbatim. After participant identifiers were removed, another member of the research team (JD) reviewed a random sample of 15% of the transcripts for accuracy and found only a few minor typographical errors. All transcripts were then independently coded by two investigators (PCE, ALB) using an inductive content analytic approach. [56] The aim of this strategy was to descriptively summarize the information to ensure the ‘best fit to the data’. [57] We used both open and axial coding in our data analysis: open coding to develop concepts from the data, and axial coding to relate these codes (or concepts) to one another followed by the identification of themes, sub-themes and representative quotes. [27]
The two investigators undertaking coding of transcripts met three times throughout the analysis (i.e., after every seven to eight interviews) to compare themes and arrive at a final, agreed-upon set of themes through discussion. We organized these themes into tabular form and selected representative quotations for each theme/sub-theme. [27] We created joint display tables as part of our data integration procedures (Figure 1), and our qualitative and quantitative results were further combined using contiguous narrative and weaving approaches. [27, 55] We then drew upon our qualitative and quantitative results jointly to come to a set of conclusions (i.e., ‘meta-inferences’). [27]
Results
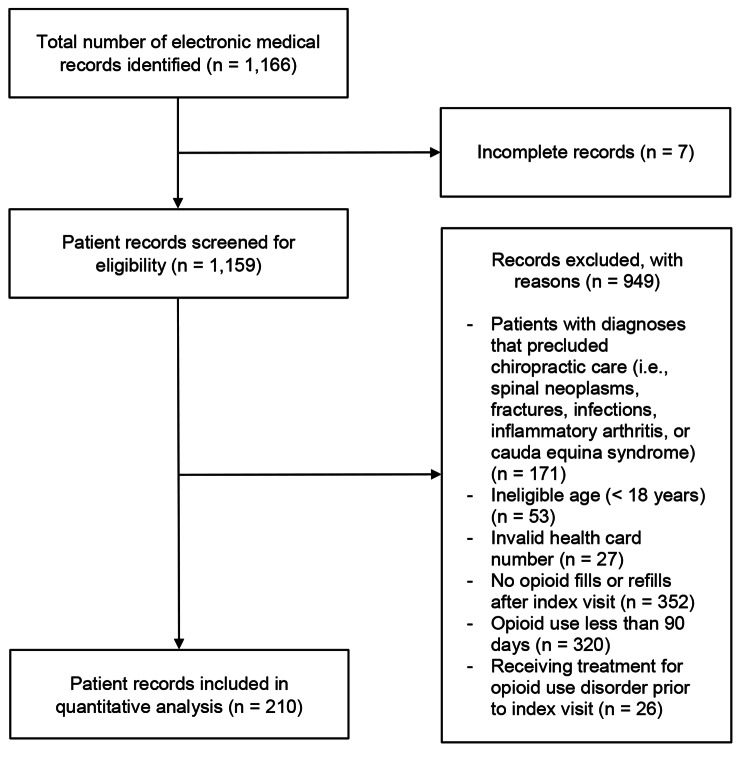
Figure 2 Quantitative findings
We identified a total of 1,166 patient records, and 210 met eligibility criteria for inclusion in our quantitative analysis (Figure 2).
Cohort characteristics
The majority (70%) of patients were ≥ 45 years of age, over half (58%) were female, approximately one-third (36%) were smokers, and 18% were obese. Patients presented with high rates of co-morbid conditions including cardiovascular disease (65%), depression (55%), anxiety (42%), diabetes (29%), and fibromyalgia (11%). The median number of healthcare visits per patient over 12 months was 5 (inter-quartile range [IQR], 2 to 8), and 23% received chiropractic services. In terms of opioid use, the median number of unique opioid fills over 12-month follow-up was 2 (IQR, 1 to 2), the median number of 30-day (or equivalent) opioid refills was 4 (IQR, 1 to 12), and baseline opioid dosage ranged from 2 to 840 mg MED (median = 30; IQR, 15 to 67 mg MED). Chiropractic recipients had similar baseline characteristics to those who did not receive chiropractic services (Additional file 6).
Quantitative analysis

Table 1 In our adjusted regression analysis, we found inverse associations between receipt of chiropractic care and filling an opioid prescription (IRR = 0.66; 95% CI, 0.52 to 0.83) or refilling an opioid prescription (IRR = 0.27; 95% CI, 0.17 to 0.42) (Table 1). There was no difference in the odds of being prescribed a higher dose of opioids (i.e., ≥ 50 mg MED) between chiropractic recipients and non-recipients at baseline (OR = 0.61; 95% CI, 0.26 to 1.47); however, chiropractic recipients were less likely to receive a higher opioid dose compared to non-recipients at three months (OR = 0.14; 95% CI, 0.04 to 0.47), six months (OR = 0.14; 95% CI, 0.05 to 0.40), nine months (OR = 0.19; 95% CI, 0.07 to 0.57), and 12 months (OR = 0.22; 95% CI, 0.08 to 0.62). At 12-month follow-up, 29 of 49 (59%) chiropractic recipients had discontinued using opioids compared to 50 of 161 (31%) non-recipients.
Patients with an index visit date in a more recent calendar year also had a lower rate of opioid refills (IRR = 0.82; 95% CI, 0.73 to 0.93) and were less likely to be receiving higher dose opioids at three months (OR = 0.73; 95% CI, 0.57 to 0.94) and six months (OR = 0.78; 95% CI, 0.62 to 0.99) (Additional file 7 [b, d, e]).
Those with a higher frequency of healthcare visits were more likely to have a higher rate of opioid refills (IRR = 1.06; 95% CI, 1.02 to 1.09) and to be receiving higher dose opioids at three months (OR = 1.11; 95% CI, 1.02 to 1.21), six months (OR = 1.09; 95% CI, 1.01 to 1.18), nine months (OR = 1.10; 95% CI, 1.02 to 1.19), and 12 months (OR = 1.12; 95% CI, 1.03 to 1.21) (Additional file 7 [b, d-g]).
Male sex, depression, and fibromyalgia were positively associated with opioid dosage at various time points (Additional file 7 [c-e]).
Contrary to our predictions, anxiety and obesity were negatively associated with opioid dosage (Additional file 7 [c, d, f]), while younger age was not associated with opioid use in our patient sample (Additional file 7). All VIFs were less than 1.4, suggesting no important multicollinearity among independent variables.
Qualitative and mixed methods findings
Twenty-three patients were recruited for interviews and 14 participated. Five patients scheduled interviews but cancelled (two chiropractic recipients, three non-recipients), two scheduled interviews but did not attend (one recipient, one non-recipient), one declined for health reasons and one was not interested. Of those who were interviewed, eight were chiropractic recipients and six were non-recipients. Among GPs, four of six medical doctors and five of six nurse practitioners completed interviews. Two medical doctors declined participation because of lack of time, and one nurse practitioner expressed interest but did not respond to further interview requests. In total, 23 interviews were completed (14 patients, nine GPs). The median durations of interviews were 25 min (range, 19 to 56) for patients and 38 min (range, 20 to 40) for GPs.
The majority (79%) of the 14 patients we interviewed were female, most (86%) were either receiving disability benefits or were unemployed, and the majority (71%) had previously received at least one opioid prescription for chronic non-cancer spinal pain. The median dosage for those currently receiving opioid medications was 19 mg MED (range, 14 to 90). Among patients and GPs, there was a large range of ages (33 to 82) and number of years attending the Langs CHC (patients: 2 to 43) or years in practice (GPs: 1 to 26), demonstrating variability among participants (Additional file 8).
Among all 23 participants, one non-chiropractic patient and four GPs made minor revisions to clarify statements from their interviews during member-checking. No other participants requested content changes or corrections to their transcripts or results. We determined that data saturation had been reached when only two new codes emerged from chiropractic recipient interviews 6, 7 and 8 (with no new codes from interviews 7 and 8); only one new code emerged from non-recipient interview 4 (with no new codes from interviews 5 and 6); and only one new code emerged from GP interviews 7, 8 and 9. At this point, participant recruitment was concluded.
Coding tree
Table 2
Table 3 We identified 37 codes across interviews which were categorized into four major themes:
(1) patient self-efficacy,
(2) accessibility of non-pharmacological services,
(3) stigma regarding use of opioids, and
(4) impact of treatment.Codes pertaining to patient self-efficacy were stratified into two sub-themes, ‘active versus passive approaches’ and ‘resistance to taking medication.’ This latter sub-theme was common among chiropractic patients. For our second theme, we created the sub-themes ‘lack of access to non-pharmacological treatment options’ and ‘access to chiropractic services at the Langs CHC.’ Lack of access to non-pharmacological services (e.g., chiropractic, physiotherapy) was identified in nearly all (21 of 23) participant interviews and was reported as a common facilitator of opioid use. Our third theme captured codes related to the opioid crisis such as negative media coverage or lived experiences. Some patients also expressed a sense of judgement from others for using prescription opioids. The remaining codes related to patients’ or GPs’ perspectives on the impact of treatment for chronic non-cancer spinal pain, including sub-themes of pain relief, functionality, recognition of the limited effectiveness of opioids for chronic pain, and anxiety and fear surrounding opioid withdrawal. Descriptions and frequency counts of each of our major themes, sub-themes, and representative participant quotes are provided in Additional file 9. Our main quantitative findings are presented with qualitative data as joint displays in Tables 2 and 3.
Discussion
Among patients receiving long-term opioid therapy for chronic non-cancer spinal pain, we found that initiating chiropractic care was associated with fewer fills and refills for prescription opioids and, when prescribed, reduced dosage of opioids. Based on our qualitative findings, use of opioids was influenced by patients’ self-efficacy and concerns about opioid-related harms, recognition of the limited effect that opioids may have on chronic pain, increasing stigma regarding use of opioids, and access to non-pharmacological treatment options.
Our findings are supported by other uncontrolled observational studies. [22–24] A retrospective analysis of quality assurance data from a CHC in Manitoba, Canada [23] found that patients referred for chiropractic services had a 22% decrease in the number of opioid tablets used after attending an average of five chiropractic visits. Between baseline and discharge, the number of chiropractic patients prescribed opioids within this health care centre decreased 26%. [23] Findings of reduced opioid usage among patients receiving chiropractic services in US Veteran Administration [22] and CHC [24] clinic settings have also been recently reported.
The integration of quantitative and qualitative methods in our study generated several insights into our results. As highlighted in our interviews, patients who were referred for chiropractic services at the Langs CHC may have been more resistant to taking opioid medication than patients not referred for chiropractic services, a sentiment supported by some published evidence. [58] In addition, GPs indicated that access to chiropractic treatment gave them another non-opioid pain management option. Lack of access to non-pharmacological services (e.g., chiropractic, physiotherapy) was reported by several participants as a facilitator of opioid use, while chiropractic patients and GPs identified negative stigma associated with the use of opioids as a common barrier.
We also found in our cohort that the proportion of chiropractic recipients who discontinued using opioids was nearly double that of non-recipients. These factors may help explain why chiropractic recipients obtained fewer opioid prescriptions and were less likely to be receiving higher opioid doses up to one year after presentation.
Similar to previous research [42, 44], we found that a higher frequency of healthcare visits was positively associated with opioid use. Patients with lower self-efficacy or experiencing greater difficulty coping with their pain may have been more likely to visit their healthcare providers more often and obtain opioid prescriptions on a more frequent basis and at higher doses. Recent evidence suggests that active pain self-management programs that include exercise, goal setting, education, and counselling on opioid discontinuation, as well as interventions aimed at supporting prescribers’ adherence to guidelines (e.g., chart audits, tracked performance metrics related to high-dose prescribing), can increase the likelihood of patients reducing their opioid dose or discontinuing opioid treatment. [59] However, as was frequently mentioned by both GPs and patients in our interviews (see Theme #2 in Additional file 8), accessibility of non-pharmacological treatment options remains a challenge, particularly for persons who are unemployed or from low income backgrounds. [26, 34–40, 42–44, 59]
We found that patients with an index visit date in a more recent calendar year had fewer opioid prescription refills and were less likely to receive higher opioid doses at 3- and 6-month follow-up. Current guidelines [13, 60] recommend optimization of non-opioid and non-pharmacologic treatments prior to opioid use, while limiting opioid doses (when first used with patients) to less than 50 mg MED, and offering a trial of voluntary tapering if doses are already ≥ 90 mg MED. Accordingly, several GPs indicated in their interviews that a concerted effort, in the form of internal chart audits and clinical team meetings, had been made in recent years to reduce opioid prescribing at the Langs CHC. When controlling for calendar year in our analyses, however, we found that the number of opioid fills, refills, and dosages were still considerably lower among chiropractic recipients.
Several observational studies have reported an association between use of chiropractic services and reduced opioid prescribing [17–21, 61] or reduced opioid use. [22–24] Previous observational research [34–39] also suggests that integrating chiropractic services with physician management of spine-related pain is associated with improved patient outcomes and potential for cost savings (e.g., reductions in advanced imaging, GP visits, and specialist referrals). When accessed as a first-line treatment, chiropractic services may also help to delay, and in some cases prevent, opioid prescription. [17–21, 61] In one of our interviews (see Theme #2, first sub-theme, Additional file 8 ), the following GP expressed that,“…having access to any kind of additional modalities in a timely and efficient manner … would probably reduce the need for opioids in the first place.”
-- GP 9Our findings add to a growing body of observational evidence that suggests integration of chiropractic services into primary care centres [] [23, 24, 34–39] and interdisciplinary spine care pathways [62] would reduce barriers to access and potentially reduce use of opioids among patients with chronic non-cancer spinal pain. However, since the efficacy of non-pharmacological interventions including chiropractic care for reducing opioid use remains uncertain [59], and observational research is susceptible to selection bias and confounding [63], well-designed randomized controlled trials are needed to confirm these findings.
Our qualitative findings suggest that lower opioid use is also related to factors such as self-efficacy and concern about opioid-related harms, access to non-pharmacological care, stigma, and knowledge of opioid effectiveness on chronic pain. Future research should investigate these factors further to inform their association with opioid use.
Strengths and limitations
Our study has several strengths. First, we used patient health card numbers to link EMR data with medical drug claims data from the Narcotics Monitoring System database at ICES to verify patient opioid prescriptions and dosages. Second, we specified the anticipated direction of association for each independent variable in our regression models a priori to provide greater confidence in our findings. Third, we used GEEs to account for hierarchical clustering and to control for differences in confounding factors between our exposed (receipt of chiropractic care) and unexposed groups. To account for policy changes in opioid prescribing, we controlled for calendar year in our analyses. This helped to more clearly delineate between a reduction in opioid use associated with access to chiropractic services versus confounding by policy change. Additional strengths included limited missing data (< 1%), direct data export from the EMR to avoid extraction errors [28], and validation of our qualitative data via member-checking. A final strength of our study is our qualitative findings, which provided a richer understanding of the barriers and facilitators to opioid use and how chiropractic services may have been used by patients and GPs to reduce reliance on opioid prescribing for chronic non-cancer spinal pain.
Our study also has several limitations. Due to the retrospective design in our quantitative phase, certain variables that may be associated with opioid use were unavailable. For example, due to the constraints of data recorded in the Langs EMR, we were unable to extract information on co-interventions that patients may have received outside of the CHC, as well as baseline severity/chronicity of patients’ spine-related pain, and additional potential confounders such as employment status or other mental health and pain conditions. However, Langs CHC patients are unlikely to access private healthcare services elsewhere due to socioeconomic disadvantages. [23–26, 34–40]
In addition, we used receipt of opioid prescriptions over three consecutive months, combined with multiple clinic visits for a non-cancer spinal pain diagnosis at the Langs CHC, as a proxy for chronic non-cancer spinal pain. Another limitation is that despite restricting our EMR data extraction to patient encounters related to non-cancer spinal pain, and only including opioid medications prescribed on or between these visit dates, it remains possible that opioids may have been prescribed for other indications. However, this would have attenuated the association between chiropractic care and opioid use. [64]
Furthermore, our primary outcome measures (i.e., opioid prescriptions and dosages) are surrogates for patient-important outcomes such as functional improvement or pain reduction. An inherent limitation with using a sequential mixed methods design (i.e., quantitative followed by qualitative) is that 11 months elapsed between our quantitative and qualitative study phases, subsequently limiting our qualitative data collection. For instance, some individuals whom we attempted to recruit from the larger cohort were no longer available for interviews (e.g., moved out of city, phone number no longer in service, or were deceased). A further limitation of the qualitative phase of our study is that we did not pilot-test our interview guides. However, one week before the interviews, participants received an information letter containing examples from the interview questions. Lastly, chiropractors engaged to provide care at the Langs CHC were selected for their focus on evidence-based, time-limited management of musculoskeletal complaints [25, 34]; practice variability among chiropractors in Canada [65] may reduce the generalizability of our findings in other settings.
Conclusion
We found that patients with chronic non-cancer spinal pain who received chiropractic care obtained fewer and lower dose opioid prescriptions than patients who did not receive chiropractic care. Follow-up interviews suggested this relationship was influenced by patient self-efficacy and concerns about opioid-related harms, limited effectiveness of opioids for chronic pain, stigma regarding use of opioids, and access to non-pharmacological treatment options. Although overall results are promising, large rigorously-conducted randomized controlled trials are needed to establish the role of chiropractic care in reducing opioid use for chronic spinal pain.
Appendix.
Additional files 1-9 (61.2KB, docx)
Additional file 1. Good Reporting of A Mixed Methods Study (GRAMMS) checklist.
Additional file 2. Morphine equivalents daily conversion factors.
Additional file 3. Interview guide (patients).
Additional file 4. Interview guide (general practitioners).
Additional file 5. Investigator reflexivity.
Additional file 6. Comparison of recipients versus non-recipients of chiropractic services.
Additional file 7 (a-g). Univariable and multivariable regression models for each outcome of interest.
Additional file 8. Characteristics of interview participants.
Additional file 9. Qualitative themes generated from semi-structured interviews.Acknowledgements
This study contracted ICES Data & Analytic Services (DAS) and used de-identified data from the ICES Data Repository, which is managed by ICES with support from its funders and partners: Canada’s Strategy for Patient-Oriented Research (SPOR), the Ontario SPOR Support Unit, the Canadian Institutes of Health Research, and the Government of Ontario. The opinions, results, and conclusions reported are those of the authors. No endorsement by ICES or any of its funders or partners is intended or should be inferred.
The authors also wish to acknowledge Jomin Joseph, Decision Support Specialist at Compass Community Health, for his invaluable assistance with the electronic medical record data extraction for this project.
List of abbreviations
AIC = Akaike Information Criterion
CHC = Community Health Centre
CI = Confidence Interval
COREQ = Consolidated Criteria for Reporting Qualitative Research
DC = Doctor of Chiropractic
EMR = Electronic Medical Record
GEE = Generalized Estimating Equation
GP = General Practitioner
GRAMMS = Good Reporting of A Mixed Methods Study
ICES = Institute for Clinical Evaluative Sciences
IQR = Inter-quartile range
IRR = Incidence Rate Ratio
MAXQDA = Max Weber Qualitative Data Analysis
MED = Morphine Equivalents Daily
OR = Odds Ratio
QIC = Quasi-likelihood under the Independence model Criterion
SPSS = Statistical Package for the Social Sciences
STROBE = Strengthening the Reporting of Observational Studies in Epidemiology
US = United States
VIF Variance Inflation Factor
Authors’ contributions
Concept development: PCE, MO, LM, JWB;
Design: PCE, MO, LM, JWB;
Supervision: MO, LM, JWB;
Methods consultation: MO, LM, JWB;
Data collection/processing: PCE, ALB, DFC, JD;
Analysis/interpretation: PCE, ALB;
Literature search: PCE;
Writing of manuscript:
PCE; Critical review of manuscript for intellectual content: PCE, ALB, MO, LM, DFC, JD, JWB.
All authors read and approved the final manuscript.
Funding
This work was supported by the Canadian Chiropractic Research Foundation (grant number 2020-03).
Availability of data and materials
The dataset from this study is held securely in coded form at the Institute for Clinical Evaluative Sciences (ICES). While data sharing agreements prohibit ICES from making the dataset publicly available, access may be granted to those who meet prespecified criteria for confidential access, available at www.ices.on.ca/DAS. The full dataset creation plan and underlying analytic code are available from the corresponding author (PCE) upon reasonable request, understanding that the computer programs may rely upon coding templates or macros that are unique to ICES and are therefore either inaccessible or may require modification.
Competing interests
PCE is supported by research grants from McMaster University and the NCMIC Foundation for graduate studies outside of the submitted work.
All authors have no other conflicts to declare.

References:
Dahlhamer J, Lucas J, Zelaya C, Nahin R, Mackey S, DeBar L.
Prevalence of Chronic Pain and High-Impact Chronic Pain
Among Adults — United States, 2016
MMWR Morb Mortal Wkly Rep 2018 (Sep 14); 67 (36): 1001-1006van Hecke O, Torrance N, Smith BH.
Chronic pain epidemiology and its clinical relevance.
Br J Anaesth. 2013;111(1):13–8.
doi: 10.1093/bja/aet123.Breivik H, Collett B, Ventafridda V, Cohen R, Gallacher D.
Survey of Chronic Pain in Europe: Prevalence,
Impact on Daily Life, and Treatment
European J Pain 2006 (May); 10 (4): 287-333Sá KN, Moreira L, Baptista AF, Yeng LT, Teixeira JM.
Prevalence of Chronic Pain in Developing Countries:
Systematic Review and Meta-analysis
Pain Rep 2019 (Dec 6); 4 (6): e779Ramage-Morin PL.
Chronic pain in Canadian seniors.
Health Rep. 2008;19(1):37–52Ramage-Morin PL, Gilmour H.
Chronic pain at ages 12 to 44.
Health Rep. 2010;21(4):53–61Cohen SP, Vase L, Hooten WM.
Chronic pain: an update on burden, best practices,
and new advances.
Lancet. 2021;397(10289):2082–97.
doi: 10.1016/S0140-6736(21)00393-7Canadian Pain Task Force Report. March 2021.
An Action Plan for Pain in Canada 2021
Health Canada
Address Locator 0900C2
Ottawa, ON K1A 0K9Steglitz J, Buscemi J, Ferguson MJ.
The future of pain research, education, and treatment:
a summary of the IOM report “Relieving pain in America:
a blueprint for transforming prevention, care,
education, and research”.
Transl Behav Med. 2012;2(1):6–8.
doi: 10.1007/s13142-012-0110-2International Narcotics Control Board.
Narcotic drugs: Estimated world requirements for 2020; 2019.
https://www.incb.org/documents/Narcotic-Drugs/Technical-
Publications/2019/Narcotic_Drugs_Technical_Publication_
2019_web.pdf
Accessed 17 Feb 2022.Busse JW, Wang L, Kamaleldin M, Craigie S, Riva JJ, Montoya L, Mulla SM, Lopes LC, Vogel N, Chen E.
Opioids for chronic noncancer pain:
a systematic review and meta-analysis.
JAMA. 2018;320(23):2448–60.
doi: 10.1001/jama.2018.18472Gomes T, Greaves S, Martins D, Bandola D, Tadrous M, Singh S, Juurlink D, Mamdani M.
Latest Trends in Opioid-Related Deaths in Ontario: 1991 to 2015.
Toronto: Ontario Drug Policy Research Network; 2017.
https://odprn.ca/wp-content/uploads/2017/04/ODPRN-Report_
Latest-trends-in-opioid-related-deaths.pdf
Accessed 17 Feb 2022.Busse JW, Craigie S, Juurlink DN, Buckley DN, Wang L.
Guideline for Opioid Therapy and Chronic Noncancer Pain
CMAJ. 2017 (May 8); 189 (18): E659–E666Bedson J, Chen Y, Ashworth J, Hayward RA, Dunn KM, Jordan KP.
Risk of adverse events in patients prescribed long-term opioids:
a cohort study in the UK Clinical Practice Research Datalink.
Eur J Pain. 2019;23(5):908–22.
doi: 10.1002/ejp.1357.Gwira Baumblatt JA, Wiedeman C, Dunn JR, Schaffner W, Paulozzi LJ, Jones TF.
High-risk use by patients prescribed opioids for pain
and its role in overdose deaths.
JAMA Intern Med. 2014;174(5):796–801.
doi: 10.1001/jamainternmed.2013.12711.Canadian Chiropractic Association.
A Better Approach to Pain Management:
Responding to Canada’s Opioid Crisis; 2016.
https://www.chiropractic.ca/wp-content/uploads/2016/11/
A-Better-Approach-to-Pain-Management-in-Canada3-1.pdf
Accessed 17 Feb 2022.Corcoran KL, Bastian LA, Gunderson CG, Steffens C, Brackett A, Lisi AJ.
Association Between Chiropractic Use and Opioid
Receipt Among Patients with Spinal Pain:
A Systematic Review and Meta-analysis
Pain Medicine 2020 (Feb 1); 21 (2): e139–e145Kazis LE, Ameli O, Rothendler J, Garrity B, Cabral H.
Observational Retrospective Study of the Association of
Initial Healthcare Provider for New-onset Low Back Pain
with Early and Long-term Opioid Use
BMJ Open. 2019 (Sep 20); 9 (9): e028633Correction: Observational retrospective study of the association
of initial healthcare provider for new-onset low back pain
with early and long-term opioid use.
BMJ Open. 2020;10(1):e028633corr1.
Erratum for: BMJ Open. 2019;9(9):e028633Whedon JM, Toler AWJ, Kazal LA, Bezdjian S, Goehl JM, Greenstein J.
Impact of Chiropractic Care on Use of Prescription
Opioids in Patients with Spinal Pain
Pain Medicine 2020 (Dec 25); 21 (12): 3567–3573Whedon JM, Uptmor S, Toler AWJ, Bezdjian S, MacKenzie TA
Association Between Chiropractic Care and Use of
Prescription Opioids Among Older Medicare
Beneficiaries with Spinal Pain:
A Retrospective Observational Study
Chiropractic & Manual Therapies 2022 (Jan 31); 30: 5Lisi AJ, Corcoran KL, DeRycke EC, Bastian LA, Becker WC.
Opioid Use Among Veterans of Recent Wars
Receiving Veterans Affairs Chiropractic Care
Pain Medicine 2018 (Sep 1); 19 (suppl_1): S54–S60Passmore S, Manansala C, Malone Q, Toth EA, Olin GM.
Opioid usage patterns, patient characteristics, and the
role of chiropractic services in a publicly funded
inner city health care facility
Spine J. 2019;19(2019):78-9Prater C, Tepe M, Battaglia P.
Integrating a Multidisciplinary Pain Team and Chiropractic
Care in a Community Health Center: An Observational
Study of Managing Chronic Spinal Pain
J Primary Care & Community Health 2020 (Sep 10)Emary PC, Oremus M, Mbuagbaw L, Busse JW.
Association of chiropractic integration in an Ontario
community health centre with prescription opioid use
for chronic non-cancer pain:
a mixed methods study protocol.
BMJ Open. 2021;11(11):e051000.
doi: 10.1136/bmjopen-2021-051000Langs.
Cambridge: Langs Community Health Centre; 2018.
https://www.langs.org Accessed 17 Feb 2022.Creswell JW, Plano Clark VL.
Designing and Conducting Mixed Methods Research. 3.
Thousand Oaks: Sage; 2018Vassar M, Holzmann
The retrospective chart review:
important methodological considerations.
J Educ Eval Health Prof. 2013;10:12.
doi: 10.3352/jeehp.2013.10.12Greene JC, Caracelli VJ, Graham WF.
Toward a conceptual framework for mixed-method
valuation designs.
Educ Eval Policy Anal. 1989;11(3):255–74von Elm E, Altman DG, Egger M, Pocock SJ, Gřtzsche PC
STROBE Initiative The Strengthening the Reporting of
Observational Studies in Epidemiology (STROBE)
statement: guidelines for reporting
observational studies.
Ann Intern Med. 2007;147(8):573–7.
doi: 10.7326/0003-4819-147-8-200710160-00010Tong A, Sainsbury P, Craig J.
Consolidated criteria for reporting qualitative research
(COREQ): a 32-item checklist for interviews
and focus groups.
Int J Qual Health Care. 2007;19(6):349–57.
doi: 10.1093/intqhc/mzm042.O’Cathain A, Murphy E, Nicholl J.
The quality of mixed methods studies
in health services research.
J Health Serv Res Policy. 2008;13(2):92–8.
doi: 10.1258/jhsrp.2007.007074.Fŕbregues S, Hong QN, Escalante-Barrios EL, Guetterman TC.
A methodological review of mixed methods research in
palliative and end-of-life care (2014–2019)
Int J Environ Res Public Health. 2020;17(11):3853.
doi: 10.3390/ijerph17113853.Emary PC, Brown AL, Cameron DF, Pessoa AF, Bolton JE.
Management of Back Pain-related Disorders in a Community
With Limited Access to Health Care Services:
A Description of Integration of Chiropractors
as Service Providers
J Manipulative Physiol Ther 2017 (Nov); 40 (9): 635–642Garner MJ, Aker P, Balon J, Birmingham M, Moher D.
Chiropractic care of musculoskeletal disorders in a unique
population within Canadian Community Health Centers.
J Manipulative Physiol Ther. 2007;30(3):165–70.
doi: 10.1016/j.jmpt.2007.01.009.Mior S, Gamble B, Barnsley J, Côté P, Côté E.
Changes in Primary Care Physician's Management of Low Back Pain
in a Model of Interprofessional Collaborative Care:
An Uncontrolled Before-After Study
Chiropractic & Manual Therapies 2013 (Feb 1); 21 (1): 6Passmore SR, Toth A, Kanovsky J, Olin G.
Initial Integration of Chiropractic Services into
a Provincially Funded Inner City Community
Health Centre: A Program Description
J Can Chiropr Assoc 2015 (Dec); 59 (4): 363–372Manansala C, Passmore S, Pohlman K, Toth A, Olin G.
Change in Young People's Spine Pain Following Chiropractic
Care at a Publicly Funded Healthcare Facility in Canada
Complement Ther Clin Pract. 2019 (May); 35: 301–307Emary PC, Brown AL, Cameron DF, Pessoa AF.
Chiropractic Integration Within a Community Health Centre:
A Cost Description and Partial Analysis of Cost-utility
from the Perspective of the Institution
J Can Chiropr Assoc. 2019 (Aug); 63 (2): 64–79Community Health Centres.
Toronto: Ontario Ministry of Health and Long-Term Care; 2021.
https://www.ontario.ca/page/community-health-centres
Accessed 17 Feb 2022.Nolet PS, Côté P, Cassidy JD, Carroll LJ.
The association between self-reported cardiovascular
disorders and troublesome neck pain:
a population-based cohort study.
J Manipulative Physiol Ther. 2012;35(3):176–83.
doi: 10.1016/j.jmpt.2012.01.006Ritzwoller DP, Crounse L, Shetterly S, et al.
The association of comorbidities, utilization and costs
for patients identified with low back pain.
BMC Musculoskelet Disord. 2006;7:72.
doi: 10.1186/1471-2474-7-72Bath B, Trask C, McCrosky J, Lawson J.
A biopsychosocial profile of adult Canadians with and without
chronic back disorders: a population-based analysis of
the 2009–2010 Canadian Community Health Surveys.
Biomed Res Int. 2014;2014:919621.
doi: 10.1155/2014/919621Gore M, Sadosky A, Stacey BR, Tai KS, Leslie D.
The burden of chronic low back pain: clinical comorbidities,
treatment patterns, and health care costs
in usual care settings
Spine (Phila Pa 1976) 2012 (May 15); 37 (11): E668-677Robertson D, Kumbhare D, Nolet P, Srbely J, Newton G.
Associations between low back pain and depression and
somatization in a Canadian emerging adult population.
J Can Chiropr Assoc. 2017;61(2):96–105.Feingold D, Brill S, Goor-Aryeh I, Delayahu Y, Lev-Ran S.
The association between severity of depression and
prescription opioid misuse among chronic pain
patients with and without anxiety:
a cross-sectional study.
J Affect Disord. 2018;235:293–302.
doi: 10.1016/j.jad.2018.04.058Han B, Compton WM, Blanco C, Crane E, Lee J, Jones CM.
Prescription opioid use, misuse, and use disorders in U.S.
adults: 2015 National Survey on Drug Use and Health.
Ann Intern Med. 2017;167(5):293–301.
doi: 10.7326/M17-0865.Carroll LJ, Hogg-Johnson S, van der Velde G, Haldeman S.
Course and Prognostic Factors for Neck Pain in the
General Population: Results of the Bone and Joint
Decade 2000–2010 Task Force on Neck Pain and
Its Associated Disorders
Spine (Phila Pa 1976). 2008 (Feb 15); 33 (4 Suppl): S75–82Dobson AJ.
An Introduction to Generalized Linear Models. 2.
Boca Raton: Chapman & Hall/CRC; 2002.Vittinghoff E, Glidden DV, Shiboski SC, McCulloch CE.
Regression Methods in Biostatistics: Linear, Logistic,
Survival, and Repeated Measures Models. 2.
New York: Springer; 2012.Katz MH.
Multivariable analysis: a primer for readers
of medical research.
Ann Intern Med. 2003;138(8):644–50.
doi: 10.7326/0003-4819-138-8-200304150-00012Pan W.
Akaike’s information criterion in generalized
estimating equations.
Biometrics. 2001;57(1):120–5.
doi: 10.1111/j.0006-341x.2001.00120.x.Kleinbaum DG, Kupper LL, Nizam A, Rosenberg ES.
Applied Regression Analysis and Other
Multivariable Methods. 5.
Boston: Cengage Learning; 2014Collins KMT, Onwuegbuzie AJ, Jiao QG.
A mixed methods investigation of mixed methods sampling
designs in social and health science research.
J Mix Methods Res. 2007;1(3):267–94Fetters MD, Curry LA, Creswell JW.
Achieving integration in mixed methods designs –
principles and practices.
Health Serv Res. 2013;48(6 Pt 2):2134–56.
doi: 10.1111/1475-6773.12117Bradshaw C, Atkinson S, Doody O.
Employing a qualitative description approach
in health care research.
Glob Qual Nurs Res. 2017;4:2333393617742282.
doi: 10.1177/2333393617742282Sandelowski M.
Whatever happened to qualitative description?
Res Nurs Health. 2000;23(4):334–40.
doi: 10.1002/1098-240x(200008)23:4<334::aid-nur9>3.0.co;2-gHurwitz EL, Chiang LM.
A Comparative Analysis of Chiropractic and General
Practitioner Patients in North America: Findings
From the Joint Canada/United States
Survey of Health, 2002-03
BMC Health Serv Res 2006 (Apr 6); 6: 49Avery N, McNeilage AG, Stanaway F, Ashton-James CE, Blyth FM.
Efficacy of interventions to reduce long term opioid
treatment for chronic non-cancer pain:
systematic review and meta-analysis.
BMJ. 2022;377:e066375.
doi: 10.1136/bmj-2021-066375Dowell D, Haegerich TM, Chou R.
CDC guideline for prescribing opioids for chronic pain –
United States, 2016.
JAMA. 2016;315(15):1624–45.
doi: 10.1001/jama.2016.1464.Acharya M, Chopra D, Smith AM, Fritz JM, Martin BC.
Associations Between Early Chiropractic Care and
Physical Therapy on Subsequent Opioid Use Among
Persons With Low Back Pain in Arkansas
J Chiropractic Medicine 2022 (Jun); 21 (2): 67-76Zarrabian M, Bidos A, Fanti C, Young B, Drew B. V
Improving spine surgical access, appropriateness and
efficiency in metropolitan, urban and rural settings.
Can J Surg. 2017;60(5):342–8.
doi: 10.1503/cjs.016116Cook PF.
Scientific inquiry. Study designs for program evaluation:
how do we know what works?
J Spec Pediatr Nurs. 2009;14(1):70–2.
doi: 10.1111/j.1744-6155.2008.00177.xChoi BC, Noseworthy AL.
Classification, direction, and prevention of bias
in epidemiologic research.
J Occup Med. 1992;34(3):265–71.
doi: 10.1097/00043764-199203000-00010Busse JW, Pallapothu S, Vinh B, Lee V, Abril L, Canga A.
Attitudes Towards Chiropractic:
A Repeated Cross-sectional Survey
of Canadian Family Physicians
BMC Family Practice 2021 (Sep 15); 22 (1): 188

Return to OPIOID EPIDEMIC
Return to ALL ABOUT CHIROPRACTIC
Return to NON-PHARMACOLOGIC THERAPY
Return to INITIAL PROVIDER/FIRST CONTACT
Since 4-15-2026| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |