

Associations Between Early Chiropractic Care and
Physical Therapy on Subsequent Opioid Use Among
Persons With Low Back Pain in ArkansasThis section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: J Chiropractic Medicine 2022 (Jun); 21 (2): 67-76 ~ FULL TEXT
OPEN ACCESS Mahip Acharya, BPharma, Divyan Chopra, MS, Allen M. Smith, PharmD,
Julie M. Fritz, PhD, PT, Bradley C. Martin, PharmD, PhD
Division of Pharmaceutical Evaluation and Policy,
University of Arkansas for Medical Sciences,
Little Rock, Arkansas.
FROM: Kazis et. al, BMJ Open 2019
Editorial Comment: These authors are to be praised for publishing this paper. When you look at their pedigrees, it's reasonable to imagine that they may have been looking to see that physical therapy was associated with reduced opioid use. Numerous studies have shown that chiropractic already has a well-established track record for low- to no-opioid use, so they would be the perfect comparison group for a study like this. We all know that third parties are looking for safe and cost-effective alternatives to “usual care”.
In the past, a study favorable to chiropractic care, particularly one that used physical therapy as a comparison group, would never have been published, because of the long-standing medical bias against chiropractic care. So, let's tip our hats to this group of researchers for their hard work and honesty!Objective: The objective of this study was to estimate the association between early use of physical therapy (PT) or chiropractic care and incident opioid use and long-term opioid use in individuals with a low back pain (LBP) diagnosis.
Methods: A retrospective cohort study was conducted using data from Arkansas All Payers' Claims Database. Adults with incident LBP diagnosed in primary care or emergency departments between July 1, 2013, and June 30, 2017, were identified. Participants were required to be opioid naďve in the 6–month baseline period and without cancer, cauda equina syndrome, osteomyelitis, lumbar fracture, and paraplegia/quadriplegia in the entire study period. PT and chiropractic treatment were documented over the ensuing 30 days starting on the date of LBP. Any opioid use and long-term opioid use (LTOU) in 1–year follow-up were assessed. Multivariable logistic regressions controlling for covariates were estimated.
Results: A total of 40,929 individuals were included in the final sample, with an average age of 41 years and 65% being women. Only 5% and 6% received PT and chiropractic service, respectively, within the first 30 days. Sixty-four percent had incident opioid use, and 4% had LTOU in the follow-up period. PT was not associated with incident opioid use (odds ratio [OR], 1.07; 95% confidence interval [CI], 0.98–1.18) or LTOU (OR, 1.19; 95% CI, 0.97–1.45). Chiropractic care decreased the odds of opioid use (OR, 0.88; 95% CI, 0.80–0.97) and LTOU (OR, 0.56; 95% CI, 0.40–0.77).
Conclusion: In this study we found that receipt of chiropractic care, though not PT, may have disrupted the need for opioids and, in particular, LTOU in newly diagnosed LBP.
Keywords: Analgesics, Opioid; Low Back Pain; Manipulation, Chiropractic; Physical Therapy Modalities.
From the FULL TEXT Article:
Introduction
Based on data from the 2016 National Health Interview Survey, approximately 50 million U.S. adults report having chronic pain and 19.6 million additional U.S. adults report severe chronic pain that significantly interferes with daily life activities. [1] As a result of the growing popularity in opioid analgesics for pain management, opioid prescriptions have increased drastically in the previous 2 decades. Despite a recent downward trend in opioid prescribing, rates in 2015 were still 3 times higher than prescribed in 1999. [2, 3] Misuse, abuse, and overdose increased proportionately with the rise in opioid prescribing, reaching levels now considered “epidemic.” [4] More than 47,000 opioid-related deaths were reported in 2018 alone. [5]
Low back pain (LBP) is the most common noncancer pain complaint for which opioids are prescribed. [6] About 80% of adults have at least 1 LBP episode in their lifetime and LBP is among the most common reasons for a physician visit in the United States. [7–9] Furthermore, the point prevalence of chronic LBP in adults between the ages of 20 and 69 years was estimated at 13.1%. [10] Despite the lack of compelling evidence, [11, 12] between a quarter to a half of patients newly consulting a primary care provider for LBP receive an opioid prescription. [13–15]
According to data collected from the 2013 and 2014 National Health and Nutrition Survey, nearly 80% of opioid users take their pain medication long-term. [16] Long-term opioid use (LTOU) often begins with a prescription to a previously opioid-naďve individual for an acute pain condition such as LBP, [17] and several studies have demonstrated how opioids that are prescribed over an extended period of time influences risk of misuse and overdose. [18, 19] Compared with short-term use, LTOU increases the risk of opioid use disorders 5– to 40–fold depending on dose, prompting greater attention on guidelines and standards for initial prescribing. [19] Several studies have focused on prescribing patterns surrounding opioid initiation, finding the type of opioid prescribed (short- or long-acting), the days’ supply, the cumulative dose, the number of physician visits and the number of fills in the first month of initiation predict LTOU. [20–25] However, little research has focused on the use of nonpharmacological treatment services in pain management as a strategy to reduce LTOU risk, and preliminary studies aimed at examining care by physical therapists (PTs) and chiropractors consistently show a moderate to strong association between early care visits and lower LTOU risk. [26–28] However, there is a lack of research that examines both of these services when studying early care decisions in the reduction of opioid initiation and LTOU.
Chiropractors and PTs are both commonly used to manage nonspecific low back pain. Physical therapists have historically been oriented to restoring normal movement through manipulation, exercise, and stretching, while chiropractors have historically focused on manipulation to improve function of the spine to alleviate back pain. Over the past several decades, the practice choices and attitudes of PT and chiropractic care providers have converged toward a multimodal care approach that follows current clinical practice guidelines for musculoskeletal pain treatment. [29–31] For instance, providers in both professions tend to follow similar diagnostic criteria and use the same evidence-based treatment modalities for in-office and home exercise, soft-tissue therapy, patient education, and manual therapy. [29, 30, 32, 33] Unsurprisingly, most studies find PTs and chiropractors to be similarly effective for the treatment of LBP. [34, 35] However, PT and chiropractic practices are not identical in the United States, and few studies have evaluated the subtle differences in the standards of practice (eg, utilization rates of radiographic imaging, prioritization of treatment modalities) and patient perceptions of care that can potentially affect patient outcomes. [29, 33, 34, 36] For instance, 1 study evaluating the sociodemographic differences between patients who either seek chiropractic care or PT care found that chiropractic care is associated with a higher self-rating of health status and less reported days of disability (missed work, school, or bedridden owing to condition). [37] Yet, it is unknown how physical therapy and chiropractic care may influence the use of opioids in patients with LBP.
Therefore, the objective of this study was to identify the influence of early treatment with either PT or chiropractic care on opioid initiation and LTOU among patients with LBP. We hypothesized that the use of either PT or chiropractic care in the early treatment of LBP would result in a decrease in the rate of both opioid initiation and LTOU. Research focused on early care decisions involving nonpharmacological treatment options may aid practitioners by providing further insight into the comparative efficacy of different physical treatment modalities in reducing opioid use.
Materials and Methods
Data Source
The Arkansas All Payers’ Claims Database from January 2013 through June 2018 was used for this study. The Arkansas All Payers’ Claims Database is a deidentified state-level database of medical, pharmacy, and dental claims from both public and private health plans. [38] The database also contains information on enrollment status, type of health plan, and sociodemographic characteristics of insured individuals. The data were acquired through the Arkansas Biosciences Institute at the University of Arkansas for Medical Sciences and this study was determined to be exempt from human subject research by the University of Arkansas for Medical Sciences institutional review board.
Study Design and Cohort Selection
A retrospective cohort study design was used. We identified enrollees in Medicaid or commercial health plans with an incident LBP diagnosis in the primary care or emergency department (ED) between July 1, 2013 and June 30, 2017. LBP was identified examining both primary and secondary ICD-9-CM and ICD-10-CM diagnosis codes indicative of LBP (see supplemental file). The first visit with LBP diagnosis was considered the index date. To focus the analysis on adults who will not age up to Medicare and are cancer free and opioid naďve before their LBP diagnosis, the following inclusion and exclusion criteria were applied. Individuals had to be between 18 and 63 years of age at the index date continuously enrolled with both medical and pharmacy benefits for 6 months before and 12 months after the index date. The 6–month period before the index date was considered the baseline period, and the 1 year after the index date was the follow-up period. Individuals were excluded if they had any opioid prescription in the baseline period or had a cancer, osteomyelitis, cauda equina, lumbar/pelvic fracture, or quadriplegia/paraplegia diagnosis in the baseline or follow-up period. Individuals whose first opioid prescription in the follow-up was suboxone (buprenorphine-naloxone) also were excluded. Finally, individuals for whom sex was missing in the Arkansas All Payers’ Claims Database also were excluded.
Study Measures
The main variables of interest were the receipt of PT or chiropractic care on, or within 30 days after, the index LBP diagnosis. Receipt of PT or chiropractic care was assessed individually as well as in a composite measure of receiving either type of care by examining the CPT-4 codes (see supplemental file) in inpatient or outpatient claims with a primary or secondary diagnosis for LBP. The use of lumbar radiographs, lumbar advanced imaging and lumbar injections, and ED and physician office visits where a LBP diagnosis was recorded also were assessed in the 30–day window after the index date using the CPT-4 codes described in the supplemental file. Demographics (age and sex), health system (payer type), year of index diagnosis, baseline mental health comorbidities (mood disorders, schizophrenia, anxiety, personality disorders, and acute reactions to stress), substance use disorders (tobacco, opioid, and other) and a general measure of comorbidity assessed by the Charlson score were created by searching claims for diagnosis codes in the 6–month baseline period. [39] Additional covariates describing baseline use of nonsteroidal anti-inflammatory drugs, benzodiazepines, skeletal muscle relaxants, and oral steroids in the baseline were recorded by searching the prescription claims files. The main outcome measures were any opioid use and LTOU. Any opioid use was characterized in the 14–day follow-up period and the 1–year follow-up period after the index LBP diagnosis by searching for any oral opioid analgesic formulations. LTOU was identified in the 1–year follow-up period. LTOU was defined as receiving a total supply of 90 or more days of opioids in any 180–day period without a gap of more than 30 days. An alternative definition used in sensitivity analyses to define LTOU is receiving a ≥120–day supply of opioids, or receiving a ≥90 supply with 10 or more separate prescription dispensings.
Statistical Analysis
Bivariate analyses were conducted between PT and chiropractic care and the opioid use outcome measures using χ2 tests. Separate multivariable logistic regression analyses among PT, chiropractic care, and the composite PT-chiropractic care as exposures with any opioid use and LTOU were estimated adjusting for demographic and clinical variables. Odds ratio (OR) and 95% confidence intervals (CI) are reported from the multivariable regressions. The variables included in the model were based on clinical knowledge and past evidence, and no variable selection techniques were used. A correlation matrix between all covariates and variance inflation factors were estimated to detect multicollinearity. SAS version 9.4 (SAS Institute, Cary, North Carolina) was used for all analyses.
Results

Table 1
Table 2
Table 3
Table 4
Table 5 There were 253,388 unique individuals with at least 1 LBP diagnosis in the primary care or ED setting between July 2013 and June 2017 (Table 1). After applying the inclusion and exclusion criteria, there were 40,929 cancer-free patients with LBP without prior opioid use who had continuous enrollment for at least 18 months. The average age of the sample was 41 years (standard deviation = 12.61), 65% were female and 80% had commercial insurance (Table 2). The most common mental health conditions were mood disorders (26%) and anxiety disorders (26%), and 21% had nicotine dependence diagnosed. Nineteen percent had nonsteroidal anti-inflammatory prescriptions in the baseline period, and 14% filled at least 1 benzodiazepine prescription in the baseline period. A little more than a third of participants had some lumbar imaging within 30 days of the initial LBP diagnosis, with 34% having a lumbar radiograph and 0.5% having a lumbar MRI or CT.
The use or PT and chiropractic care for LBP was relatively low. Only 11% of participants used either PT or chiropractic care within 30 days of receiving a LBP diagnosis; 5% of the sample used PT and 6% used chiropractic care. Thirty percent of the sample had at least 1 opioid prescription within 14 days of index date and 54% ultimately had 1 or more opioid prescriptions in the 1–year follow-up. Among all opioid users, 64% had their first opioid prescription of less than or equal to 7 days supplied, and 10% had first opioid script with greater than 21 days’ supply. 1,805 individuals (4%) had LTOU, using the main definition. With the sensitivity definition, 1,951 individuals (5%) had LTOU.
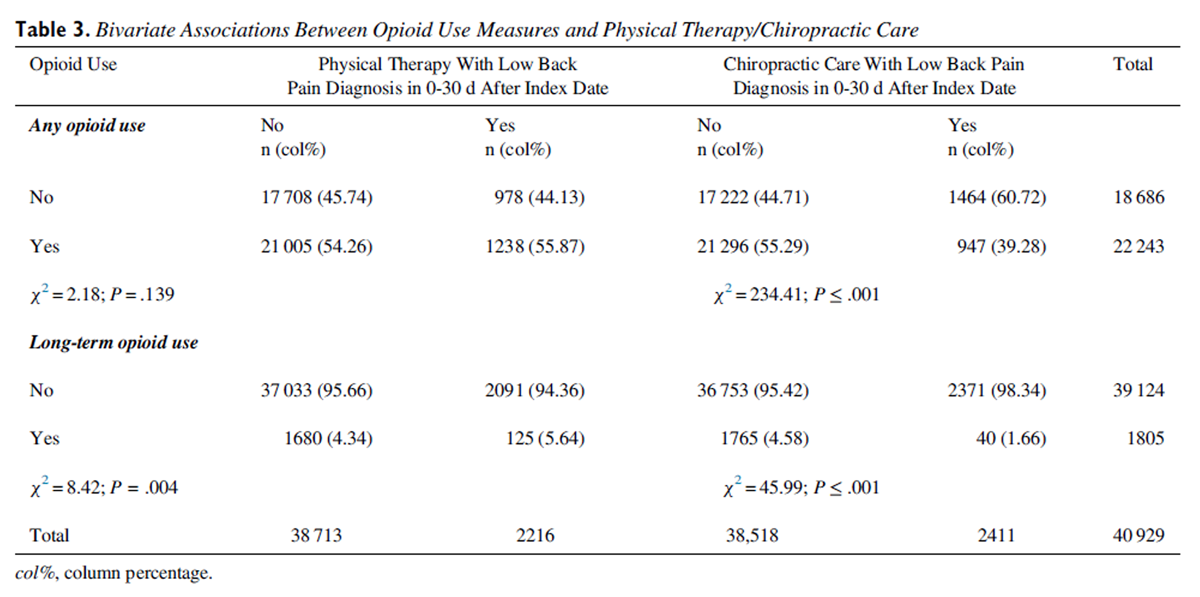
The use of PT in first 30 days was not associated with any opioid use (PT Yes = 55.87%, PT No = 54.26%; P = .139); however, those who had PT were more likely to transition to LTOU (PT Yes = 5.64%, PT No = 4.34%; P = .004) in unadjusted bivariate analyses (Table 3).
Chiropractic care, however, was associated with a lower percentage of persons using any opioids (Chiropractic Yes = 39.28%, Chiropractic No = 55.29%; P < .0001) and LTOU (Chiropractic Yes = 1.66%, Chiropractic No = 4.58%; P < .0001) in unadjusted bivariate analyses.
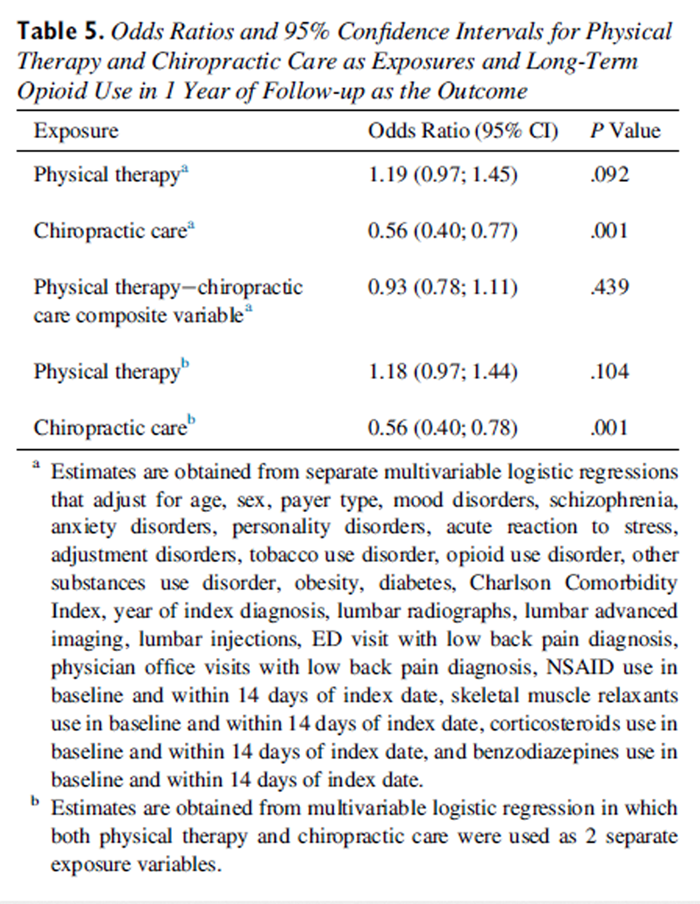
In multivariable adjusted analyses, similar relationships were observed. PT was not associated with either any opioid use (OR, 1.07; 95% CI, 0.98–1.18) or LTOU (OR, 1.19; 95% CI, 0.97–1.45), and chiropractic care was associated with a reduction in any opioid use (OR, 0.88; 95% CI, 0.80–0.97) and a more profound reduction in LTOU (OR, 0.56; 95% CI, 0.40–0.77) (Tables 4 + 5).
These relationships were preserved when PT and chiropractic care were both entered in the multivariable model. The composite PT-chiropractic care was not associated with any opioid use or LTOU (Table 5). Multicollinearity between covariates was not detected, as none of the variance inflation factors estimates exceeded 2.0.
Discussion
The use of PT and chiropractic care was low in Arkansas, with only 11% using either service within 30 days of LBP diagnosis. Only 5% used PT in this period. Compared with Western states (Alaska, Washington, Oregon, Idaho, Wyoming, and Montana) from 2009 through 2013, almost twice as many (9%) sought PT care the day of the LBP diagnosis and an additional 12% used at some time in the follow-up. [40] Three of those states had provisions for unrestricted direct access to physical therapists during the study period, meaning that a physician referral was not required to visit a physical therapist. [41, 42] As of July 2019, 5 of those 6 states had unrestricted direct access. [41] Arkansas, on the other hand, has direct access with provisions—the provisions could vary by plan and may include physician referral and visit limits, among others. [41, 43] This difference in access to PT across states may explain its low rates of utilization after LBP diagnosis in our data. Another study that used national commercial insurance data from 2007 to 2015 reported that 29% of individuals with musculoskeletal pain used PT within 90 days of diagnosis. [26] This suggests that PT may be significantly underutilized in Arkansas relative to other states.
Rates of chiropractic care use were also lower than have been reported in other populations. [44–46] A survey of Veterans with chronic noncancer pain reported that 56% of respondents reported having received chiropractic care, and 75% intended to use chiropractic care. [47] A systematic review of cross-sectional and longitudinal survey studies reported that 16% to 74% of patients with back pain received chiropractic care. [48] Several factors may explain the low rates of chiropractic care in Arkansas. First, Arkansas has the lowest density of chiropractors of approximately 2 chiropractors per 1,000 beneficiaries, which is among the lowest in the country based on Medicare claims data. [49] Another factor are the reimbursement policies for chiropractic care. Arkansas Medicaid pays for a maximum of 12 visits per year for enrollees at least 21 years of age and requires physician referral. [43] It only pays for manual manipulation of spine and does not cover other types of chiropractic services. [43] The coverage of chiropractic care in commercial insurance is plan-specific and may not be dramatically different in Arkansas than in other states. [50]
Half of the individuals with LBP had at least 1 opioid prescription in the 1–year follow-up period, and 4% to 5% had LTOU. The use of chiropractic care within 30 days of LBP diagnosis was associated with diminished use of opioids in the short term and, in particular, the long term, in which the risk of LTOU was almost cut in half. Surprisingly, the use of PT did not mitigate the risk for acute or LTOU, which is in contrast to previous studies that have found reductions in opioid use with the use of PT. [26–28, 51] For example, a study using MarketScan commercial data reported a reduction of opioid use (measured in morphine milligrams equivalent) in patients with LBP by 5% with the use of PT within 90 days of diagnosis. [26] Another study used Optum claims data, comprising commercial and Medicare Advantage enrollees, documented a 73% reduction in the odds of LTOU with the use of PT. [27] A 53% reduction in the odds of any opioid prescription was observed in Medicaid enrollees with early participation in PT. [51] The definition for PT exposure varies across studies including ours and could partially explain discrepancies in the findings. Two of the studies that report the largest reductions in opioid use required either the first visit to be a PT visit, or a PT visit on the same day as diagnosis to be considered in the PT group, [27, 49] whereas our study requires the initial encounter to be in the physician office or the ED. Examining persons with LBP who self-refer to a PT excludes LBP initially managed in the ED or physician office setting where opioids can be prescribed. Although existing observational studies are consistent in finding a reduction in opioid use with PT care, several randomized trials have failed to find differences in opioid use within 1 year between usual care and PT care groups for LBP. [52]
Existing studies on chiropractic care have reported reductions in opioid use. [46, 53, 54] A retrospective study on Veterans reported a 4–percentage point decrease in any opioid prescription within 90 days of a chiropractic visit. [55] A 50% reduction in likelihood of opioid use has been reported in retrospective claims-based studies.53,54 A clinical trial conducted in active-duty Veterans with LBP documented a 27% reduction in the odds of pain medication use. [56] A survey-based study reported that more than 80% of patients with chronic pain mentioned they derived benefit from chiropractic treatment. [57] Our results are in line with these studies and suggest, along with others, that chiropractic may help patients engage in nonpharmacologic self-care for pain despite focusing on passive interventions. [58] It may also be the case that individuals with LBP who desire to manage pain without undue reliance on medication are more likely to self-select chiropractic care. The retrospective nature of our study cannot determine if this finding represents a selection bias or treatment effect.
Limitations
Selection bias or residual confounding cannot be ruled out despite controlling for a wide range of demographics, health systems, and comorbidities. Variables such as health plan benefits design, rural-urban residence, and pain intensity could have confounded the results. For example, individuals seeking chiropractic care may have been more likely to be enrolled in health plans with more strict opioid prescribing or dispensing regulations. The low risk of LTOU in chiropractic care users could be a result of the plan-level difference instead of a causal effect of chiropractic care on back pain.
We did not assess type and duration of PT and chiropractic care used. The CPT codes used in the claims data for identifying PT and chiropractic care are not sufficiently granular to tease apart their different types. We did not evaluate outcomes such as self-reported pain or health-related quality of life, which would have provided a more complete understanding of the effects of PT and chiropractic care.
The ICD-9/10-CM codes used to identify back pain in our study may be incomplete, in particular when considering the newer ICD-10-CM codes such as M99.01–M99.04, which we did not include to identify back pain. This would have resulted in fewer persons identified for the study and may have under-assessed the frequency of PT or chiropractic care, which required a practitioner-specific CPT-4 code in addition to a back pain diagnosis. This omission is likely minor, as the most frequent ICD-10-CM codes (M54.2 and M54.5) were included and these codes are the most frequently used codes by practitioners for low back pain. [59] The study data were limited to a single state, Arkansas, which has low rates of chiropractic and PT use and high rates of opioid prescribing, and thus may not generalize to other states or nationally.
Conclusion
The use of PT and chiropractic care was low among Arkansans with LBP and with Medicaid or commercial insurance. In this sample of the population, use of chiropractic care was associated with substantial reduction in likelihood of any opioid use and LTOU, and no association was observed with PT.
Practical Applications
Utilization of chiropractic care was associated with substantial reduction in likelihood of any opioid use and long-term opioid use.
The utilization of physical therapy and chiropractic care was low among Arkansans with low back pain and with Medicaid or commercial insurance.
Physical therapy and chiropractic care may be significantly underutilized in Arkansas compared with other states.
A factor that may affect the utilization of chiropractic care and physical therapy are specialist care reimbursement policies.
Appendix. Supplementary materials
Funding Sources and Conflicts of Interest
This study was supported from funds of the UAMS Translational Research Institute grant UL1 TR003107 through the National Center for Advancing Translational Sciences of the National Institutes of Health. B.C.M. received royalties in the past 3 years from TrestleTree, LLC for the development of an opioid risk prediction tool and has received consulting fees from eMAX Health for unrelated studies.
References:
Dahlhamer J, Lucas J, Zelaya C, et al.
Prevalence of Chronic Pain and High-Impact Chronic Pain Among Adults -
United States, 2016
MMWR Morb Mortal Wkly Rep. 2018 (Sep 14); 67 (36): 1001-1006Guy GP, Zhang K, Bohm MK, et al.
Vital signs: changes in opioid prescribing in the United States, 2006-2015.
MMWR Morb Mortal Wkly Rep. 2017;66(26):697–704McCabe SE, West BT, Veliz P, McCabe V, Stoddard SA, Boyd CJ.
Trends in medical and nonmedical use of prescription opioids among US adolescents: 1976-2015Manchikanti L, Helm S, Fellows B, et al.
Opioid epidemic in the United States.
Pain Physician. 2012;15(3 suppl):ES9–E38Wilson N, Kariisa M, Seth P, Smith H, Davis NL.
Drug and opioid-involved overdose deaths — United States, 2017-2018.
MMWR Morbid Mortal Wkly Rep. 2020;69(11):290–297Jeffrey Kao MC, Minh LC, Huang GY, Mitra R, Smuck M.
Trends in ambulatory physician opioid prescription in the United States, 1997-2009.
PM&R. 2014;6(7):575–582. e4Deyo RA, Mirza SK, Martin BI.
Back pain prevalence and visit rates: estimates
from U.S. national surveys, 2002.
Spine. 2006;31(23):2724–2727Hart LG, Deyo RA, Cherkin DC.
Physician office visits for low back pain: frequency, clinical evaluation,
and treatment patterns from U.S. national survey.
Spine. 1995;20(1):11–19Licciardone JC.
The epidemiology and medical management of low back pain
during ambulatory medical care visits in the United States.
Osteopath Med Prim Care. 2008;2(1):11Shmagel A, Foley R, Ibrahim H.
Epidemiology of chronic low back pain in US Adults: data from
the 2009-2010 National Health and Nutrition Examination Survey.
Arthritis Care Res. 2016;68(11):1688–1694Chou R, Deyo R, Friedly J, Skelly A, Weimer M, Fu R, Dana T.
Systemic Pharmacologic Therapies for Low Back Pain:
A Systematic Review for an American College
of Physicians Clinical Practice Guideline
Annals of Internal Medicine 2017 (Apr 4); 166 (7): 480–492Abdel Shaheed C, Maher CG, Williams KA, Day R, McLachlan AJ.
Efficacy, tolerability, and dose-dependent effects
of opioid analgesics for low back pain.
JAMA Intern Med. 2016;176(7):958–968Fritz JM, Childs JD, Wainner RS, Flynn TW.
Primary care referral of patients with low back pain to
physical therapy: impact on future health care utilization and costs.
Spine. 2012;37(25):2114–2121Fritz JM, Brennan GP, Hunter SJ.
Physical therapy or advanced imaging as first management strategy
following a new consultation for low back pain in primary care:
associations with future health care utilization and charges.
Health Serv Res. 2015;50(6):1927–1940Rundell SD, Gold LS, Hansen RN, Bresnahan BW.
Impact of co-morbidities on resource use and adherence to guidelines
among commercially insured adults with new visits for back pain.
J Eval Clin Pract. 2017;23(6):1218–1226Mojtabai R.
National trends in long-term use of prescription opioids.
Pharmacoepidemiol Drug Saf. 2018;27(5):526–534Chou R, Turner JA, Devine EB, et al.
the effectiveness and risks of long-term opioid therapy for chronic pain:
a systematic review for a National Institutes of Health Pathways to Prevention Workshop.
Ann Intern Med. 2015;162(4):276–286Dunn KM, Saunders KW, Rutter CM, et al.
Opioid prescriptions for chronic pain and overdose.
Ann Intern Med. 2010;152(2):85Edlund MJ, Martin BC, Russo JE, DeVries A, Braden JB, Sullivan MD.
The role of opioid prescription in incident opioid abuse and dependence
among individuals with chronic noncancer pain:
the role of opioid prescription.
Clin J Pain. 2014;30(7):557–564Shah A, Hayes CJ, Martin BC.
Factors influencing long-term opioid use among opioid naive patients:
an examination of initial prescription characteristics and pain etiologies.
J Pain. 2017;18(11):1374–1383Shah A, Hayes CJ, Martin BC.
Characteristics of initial prescription episodes and
likelihood of long-term opioid use — United States, 2006–2015.
MMWR Morbid Mortal Wkly Rep. 2017;66(10):265–269Hadlandsmyth K, Lund BC, Mosher HJ.
Associations between initial opioid exposure and the likelihood for long-term use.
J Am Pharm Assoc. 2019;59(1):17–22Durand Z, Nechuta S, Krishnaswami S, Hurwitz EL, McPheeters M.
Prevalence and risk factors associated with long-term opioid use
after injury among previously opioid-free workers.
JAMA Netw Open. 2019;2(7)Zin CS, Nazar NI, Rahman NSA, Ahmad WR, Rani NS, Ng KS.
Patterns of initial opioid prescription and its association with
short-term and long-term use among opioid-naďve patients
in Malaysia: a retrospective cohort study.
BMJ Open. 2019;9(7)Deyo RA, Hallvik SE, Hildebran C, et al.
Association between initial opioid prescribing patterns and
subsequent long-term use among opioid-naďve patients:
a statewide retrospective cohort study.
J Gen Intern Med. 2017;32(1):21–27Sun E, Moshfegh J, Rishel CA, Cook CE, Goode AP, George SZ.
Association of early physical therapy with long-term opioid use
among opioid-naive patients with musculoskeletal pain.
JAMA Netw Open. 2018;1(8)Kazis LE, Ameli O, Rothendler J, et al.
Observational Retrospective Study of the Association of Initial
Healthcare Provider for New-onset Low Back Pain with Early
and Long-term Opioid Use
BMJ Open. 2019 (Sep 20); 9 (9): e028633Fritz JM, King JB, McAdams-Marx C.
Associations between early care decisions and the risk for long-term
opioid use for patients with low back pain with a new physician
consultation and initiation of opioid therapy.
Clin J Pain. 2018;34(6):552–558Beliveau PJH, Wong JJ, Sutton DA, Simon NB, Bussieres AE, Mior SA, et al.
The Chiropractic Profession: A Scoping Review of Utilization Rates,
Reasons for Seeking Care, Patient Profiles, and Care Provided
Chiropractic & Manual Therapies 2017 (Nov 22); 25: 35Bussičres AE, Zoubi F, Stuber K, et al.
Evidence-based Practice, Research Utilization, and Knowledge
Translation in Chiropractic: A Scoping Review
BMC Complement Altern Med. 2016 (Jul 13); 16 (1): 216Mota da Silva T, da Cunha Menezes, Costa L, Garcia AN, Costa LOP.
What do physical therapists think about evidence-based practice?
A systematic review.
Man Ther. 2015;20(3):388–401DeRosa CP, Porterfield JA.
A physical therapy model for the treatment of low back pain.
Phys Ther. 1992;72(4):261–269Shipton EA.
Physical therapy approaches in the treatment of low back pain.
Pain Ther. 2018;7(2):127–137Khodakarami N.
Treatment of patients with low back pain: a comparison of
physical therapy and chiropractic manipulation.
Healthcare. 2020;8(1):44Blanchette M, Stochkendahl M., Da Silva RB, et al.
Effectiveness and Economic Evaluation of Chiropractic Care for the Treatment
of Low Back Pain: A Systematic Review of Pragmatic Studies
PLoS One. 2016 (Aug 3); 11 (8): e0160037Skargren EI, Öberg BE, Carlsson PG, Gade M.
Cost and effectiveness analysis of chiropractic and physiotherapy
treatment for low back and neck pain. Six-month follow-up.
Spine. 1997;22(18):2167–2177Chevan J, Riddle DL.
Factors associated with care seeking from physicians, physical therapists,
or chiropractors by persons with spinal pain: a population-based study.
J Orthop Sports Phys Ther. 2011;41(7):467–476Arkansas All-Payer Claims Database. Available at:
https://www.arkansasapcd.net/Home
Accessed February 3, 2022.Charlson ME, Pompei P, Ales KL, MacKenzie CR.
A new method of classifying prognostic comorbidity in
longitudinal studies: development and validation.
J Chronic Dis. 1987;40(5):373–383Frogner BK, Harwood K, Andrilla CHA, Schwartz M, Pines JM.
Physical therapy as the first point of care to treat low back pain:
an instrumental variables approach to estimate impact on
opioid prescription, health care utilization, and costs.
Health Serv Res. 2018;53(6):4629–4646American Physical Therapy Association.
Levels of patient access to physical therapists services in the U.S. Available at:
https://www.apta.org/advocacy/issues/direct-access-advocacy/direct-access-by-state
Accessed September 29, 2020.Basore T.
A review of direct access to physical therapy. Available at:
http://scholarworks.gvsu.edu/honorsprojects/57
Accessed September 29, 2020.Arkansas Department of Human Services.
Helpful information for clients. Available at:
https://humanservices.arkansas.gov/divisions-shared-services/medical-services/helpful-information-for-clients/
Accessed September 29, 2020.Wade C, Chao M, Kronenberg F, Cushman L, Kalmuss D.
Medical pluralism among american women: results of a national survey.
J Women's Health. 2008;17(5):829–840Lozier CC, Nugent SM, Smith NX, et al.
Correlates of use and perceived effectiveness of non-pharmacologic
strategies for chronic pain among patients prescribed long-term opioid therapy.
J Gen Intern Med. 2018;33(S1):46–53Corcoran KL, Bastian LA, Gunderson CG, et al.
Association Between Chiropractic Use and Opioid Receipt Among
Patients with Spinal Pain: A Systematic Review and Meta-analysis
Pain Medicine 2020 (Feb 1); 21 (2): e139–e145Denneson LM, Corson K, Dobscha SK.
Complementary and alternative medicine use among veterans
with chronic noncancer pain.
J Rehabil Res Dev. 2011;48(9):1119–1128Murthy V, Sibbritt DW, Adams J.
An integrative review of complementary and alternative medicine use
for back pain: a focus on prevalence, reasons for use,
influential factors, self-perceived effectiveness,
and communication.
Spine J. 2015;15(8):1870–1883Sarpong NO, Lakra A, Jennings E, Cooper HJ, Shah RP, Geller JA.
Same-day physical therapy following total knee arthroplasty leads to
improved inpatient physical therapy performance and decreased inpatient opioid consumption.
J Arthroplasty. 2019;34(12):2931–2936Heyward J, Jones CM, Compton WM, et al.
Coverage of Nonpharmacologic Treatments for Low Back Pain
Among US Public and Private Insurers
JAMA Network Open 2018 (Oct 5); 1 (6): e183044Thackeray A, Hess R, Dorius J, Brodke D, Fritz J.
Relationship of opioid prescriptions to physical therapy referral
and participation for medicaid patients with new-onset low back pain.
J Am Board Fam Med. 2017;30(6):784–794Rhon DI, Miller RB, Fritz JM.
Effectiveness and downstream healthcare utilization for patients that
received early physical therapy versus usual care for low back pain.
Spine. 2018;43(19):1313–1321Whedon JM, Toler AWJ, Goehl JM, Kazal LA.
Association Between Utilization of Chiropractic Services for
Treatment of Low-Back Pain and Use of Prescription Opioids
J Altern Complement Med. 2018 (Jun); 24 (6): 552–556Whedon JM, Toler AWJ, Kazal LA, Bezdjian S, Goehl JM, Greenstein J.
Impact of Chiropractic Care on Use of Prescription
Opioids in Patients with Spinal Pain
Pain Medicine 2020 (Dec 25); 21 (12): 3567–3573
There are more like this at: SPINAL PAIN MANAGEMENTLisi AJ, Corcoran KL, DeRycke EC, et al.
Opioid Use Among Veterans of Recent Wars Receiving
Veterans Affairs Chiropractic Care
Pain Med. 2018 (Sep 1); 19 (suppl_1): S54–S60Goertz CM, Long CR, Vining RD, Pohlman KA, Walter J, Coulter I.
Effect of Usual Medical Care Plus Chiropractic Care vs Usual Medical Care
Alone on Pain and Disability Among US Service Members With
Low Back Pain. A Comparative Effectiveness Clinical Trial
JAMA Network Open. 2018 (May 18); 1 (1): e180105 NCT01692275Fleming S, Rabago DP, Mundt MP, Fleming MF.
CAM therapies among primary care patients using opioid therapy for chronic pain.
BMC Complement Altern Med. 2007;7(1):1–7Penney LS, Ritenbaugh C, DeBar LL, Elder C, Deyo RA.
Provider and Patient Perspectives on Opioids and Alternative Treatments
for Managing Chronic Pain: A Qualitative Study
BMC Pamily Practice 2017 (Mar 24); 17 (1): 164Coleman BC, Goulet JL, Higgins DM, et al.
ICD-10 coding of musculoskeletal conditions in the Veterans Health Administration.
Pain Med. 2021;22(11):2597–2603.
Return to OPIOID EPIDEMIC
Return NON-PHARMACOLOGIC THERAPY
Return to INITIAL PROVIDER/FIRST CONTACT
Since 8-28-2022


| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |