

Enduring Versus Curable:
Mixed-methods Perspectives About
Pain Among Chiropractic PatientsThis section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: Eur J Integr Med 2026 (May 25): 85: 102689 ~ FULL TEXT
OPEN ACCESS Margaret D Whitley • Michele Maiers • Lara Hilton • Ryan S Wexler • Ian Coulter • Praise Iyiewuare • Gery Ryan
RAND, Behavioral and Policy Sciences,
1776 Main St.,
Santa Monica, CA 90401, USA.
Introduction: Qualitative methods are fundamental for studying patient preferences, particularly to understand how people perceive and manage pain that is unresponsive to standard treatment. Yet there is limited literature describing how formative qualitative research can inform quantitative studies on chronic pain. Integrating patient perspectives from qualitative research helps ensure that quantitative protocols and pain measures are grounded in patients' lived experiences.This paper details how our team, as part of a center focused on appropriate care for spinal pain, collected qualitative data about how chiropractic patients perceived pain chronicity, and how we used these findings to inform a national quantitative study.
Methods: In this exploratory sequential mixed methods study, we conducted 40 semi-structured interviews and deployed a mixed methods survey to 108 chiropractic patients with spinal pain. We conducted thematic analysis of the qualitative data, and we summarized those findings in a visual framework. The visual framework, in turn, informed the inclusion criteria and survey items for a quantitative, observational survey of 2,025 chronic pain patients from 125 chiropractic clinics in the United States.
Results: Qualitative research revealed that many patients viewed chronic pain as permanent. Patients who defined chronicity this way shifted from seeking a cure to utilizing longer-term pain management and coping strategies; in this way, patients' understandings about chronicity influenced their care-seeking and satisfaction. This set of findings challenged our team's initial assumption that chronicity was primarily understood in terms of pain duration or intensity, and that all patients expected a cure.
Conclusions: Qualitative findings shaped the methods and interpretation of our quantitative observational research. This process led to a conceptual framework of chronic pain, more informative surveys and a shared understanding of the diverse beliefs that drive care-seeking behaviors among chronic pain patients.
Keywords: Chronic pain; Complementary and integrative healthcare; Mixed methods; Spinal pain.
From the FULL TEXT Article:
Introduction
Low back and neck pain are among the top causes of years lived with disability worldwide. [1, 2] Low back pain and neck pain affect a large share of the US population – 9.4% and 4.9%, respectively [2, 3] – and these conditions lead to decreased quality of life as well as enormous healthcare costs, with low back pain alone accounting for roughly $85 billion annually. [4]
Low back and neck pain, which we will refer to jointly as spinal pain, can be characterized as acute or chronic. [5–7] The most commonly used definitions for chronic pain are based on pain duration of longer than 3 months; [6–8] some scholars have distinguished between acute pain and chronic pain based on the frequency and patterning of the condition as well. [6] Describing a pain condition as either acute or chronic can have implications for how patients and their providers think about the problem and try to resolve it. [5–7]
Some experts state that chronic pain should not be understood as acute pain that has not resolved, but rather as a distinct pain process that may or may not begin as a symptom of some other condition. [5, 9, 10] Regardless of the definition, chronic pain is difficult to treat and often requires long term management. [11]
Chronic pain patients often must engage in one or more pain management approaches, whether self-care, professional care, or a combination of the two. [12, 13] Many patients with pain report not having an effective way to manage their condition. [14, 15] There is no single “silver bullet” treatment that relieves pain and improves function for all spinal pain patients. [16, 17]
There is instead a variety of physical, psychological, pharmacological and environmental treatment options that patients and their providers may consider, in accordance with the patients’ specific condition, needs and preferences. [12, 18] Non-pharmacological treatments, including complementary and integrative healthcare (CIH) approaches, are increasingly important to meet individual needs, while decreasing the risk of addiction stemming from prescription opioid use. [19]
Many evidence-based, non-pharmacological options for pain management are categorized as CIH, including spinal manipulative therapy, a manual therapy that is typically performed by chiropractors, [12] and is increasingly prominent in many healthcare systems. [20–22] One-third of the US population uses some kind of CIH care, [23, 24] and it is estimated that over 50% have sought care from chiropractors at some point in their lifetime. [25]
Chiropractic and other CIH patients are a large part of the overall population, but they may have distinct needs, preferences and expectations relative to non-CIH users. [26] Prior research examined how patients initiate and continue CIH care, including how they obtain referrals from their primary care providers, [27, 28] how they combine conventional and complementary care, [26] the complex emotional and healthcare journeys for patients who seek CIH and conventional care for rare conditions, [29] how delays in access to conventional care may affect patients’ tendency to seek CIH care, [30] and how patients consider physical, affective, cognitive and interpersonal aspects of CIH treatment when deciding whether to continue seeking care. [31]
Notably, little research has documented the steps that are often required for seeking chiropractic care for spinal pain. A patient’s preferences, beliefs and experiences related to their pain and to pain management will shape the approach each patient takes. In addition, clinicians and researchers need to understand those preferences, beliefs, and experiences in order to design rigorous research studies or offer compelling treatment options.
Mixed methods approaches, which combine quantitative and qualitative methods in a variety of ways, are increasingly applied in many fields, including health services research. [32] Foreground qualitative research is helpful and often essential to prepare for quantitative studies on a variety of topics. However, the nuanced ways in which qualitative research shapes later quantitative methods and informs the research team’s definitions and assumptions, is less visible in published work. [32]
Prior mixed methods work about chiropractic healthcare has examined, for instance, care seeking and satisfaction with care for Danish chiropractic patients with lumbar radiculopathy; [33] we are not aware of similar mixed methods work with a U.S. population of chiropractic, spinal pain patients. Further, there is a dearth of information about how exploratory sequential mixed methods research can be applied to better understand patients in a CIH context.
Here we document our process in collecting this information as part of a Center of Excellence for Research on CIH. We describe how we collected two forms of qualitative data about patient preferences for pain treatment and used that to inform a large quantitative survey. In addition, we identify the key structures and steps that made mixed methods research possible in this population.
Methods
The Center:
As part of a National Institutes of Health (NIH)-funded Center of Excellence for Research on CIH that began in 2014, [34] our team conducted four interrelated research studies about appropriate care for chronic spinal pain. The Center focused on studying the appropriateness of spinal manipulation (manipulative therapy) and mobilization for low back pain and neck pain.
Appropriateness of care is defined as “care that is effective (based on valid evidence), efficient (cost-effective), and consistent with the ethical principles and preferences of relevant individuals, communities or society.” [35] A major goal of the Center was to understand how individual preferences and beliefs should be taken into account when determining appropriateness. Spinal manipulative therapy and mobilization are most commonly performed by doctors of chiropractic (DCs), [36] so much of the Center’s research focused on chiropractic patients. The work described here was part of an arc of research conducted by the Center, which has been described elsewhere. [34, 37–41]
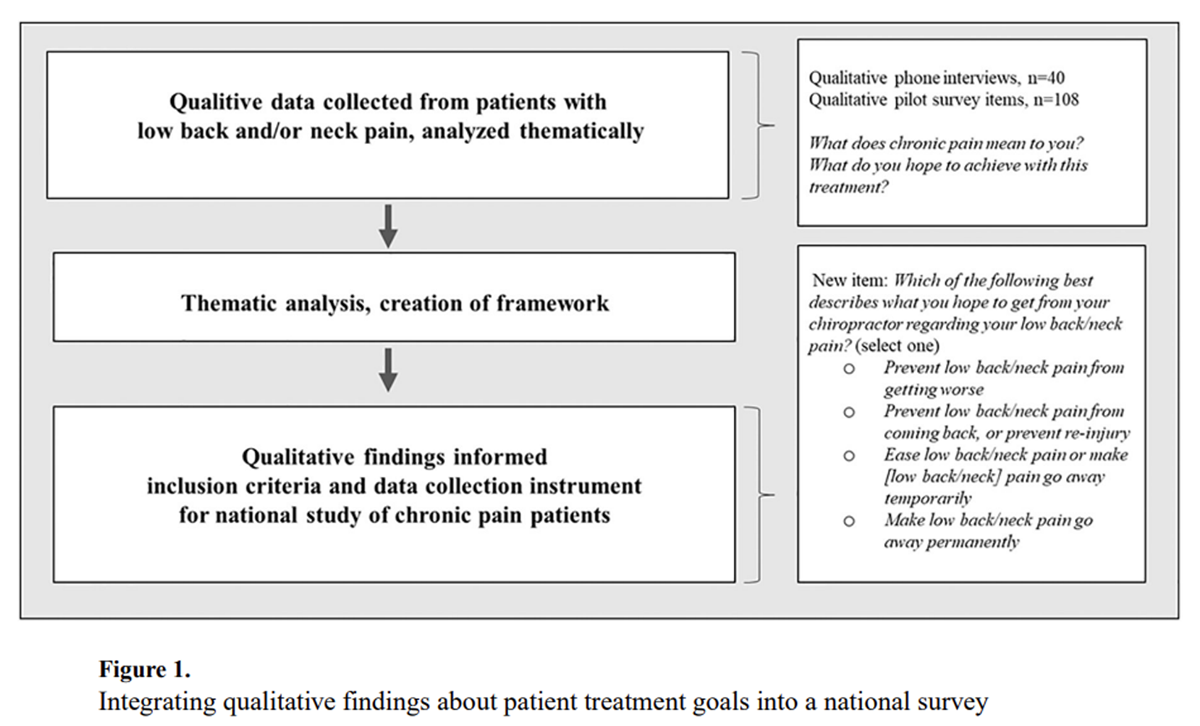
Figure 1 A primary objective of the Center was to quantitatively characterize, across a population of CIH patients, which treatments patients preferred for their spinal pain. This work was planned to begin with formative qualitative research. Other major activities for the Center included examining the costs associated with various types of chronic pain care and conducting expert panels about appropriate care for spinal pain. Figure 1 shows qualitative studies informed the national patient study and appropriateness study.
All study activities, including the qualitative and quantitative data collection described here, were reviewed and approved by RAND’s Human Subjects Protection Committee (Study # 2013–0763). The research team completed an informed consent process with all study participants. For phone interview participants, the interviewer read the consent form to participants verbally over the phone, asked whether the individual agreed to participate, and documented this response; for participants who completed an online survey, the consent form was displayed within the online survey, and participants could check a box if they agreed to participate.
Qualitative studies: Setting, sample, data collection and analysis
The Center used two qualitative studies in an exploratory sequential design [42] to inform the quantitative phase of data collection:study 1 was comprised of semi-structured phone interviews and
study 2 was comprised of qualitative items embedded in an online pilot survey.The qualitative phone interviews and pilot survey were conducted with five chiropractic clinics in Los Angeles County, California. Los Angeles’ socioeconomically and racially/ethnically diverse population, mix of suburban and urban regions, and many chiropractic clinics, allowed us to access chiropractic patients with a broad range of experiences regarding chronic spinal pain treatment.
Clinics were selected through a respondent-driven (i.e., snowball sampling) approach, starting with two clinics already known to our research team based on their interest in research. We selected five clinics representing three different regions of Los Angeles to maximize socioeconomic and racial/ethnic diversity. One clinic specialized in a small number of conditions including spinal stenosis while the other four were general chiropractic practices.Study 1 qualitative phone interviews:
The qualitative phone interviews relied on a purposive sample of 40 patients. We instructed staff at the five chiropractic clinics to inform patients with spinal pain about our study, and to collect names and contact information for up to 16 patients, per clinic, who were willing to participate. In anticipation of partial enrollment from these patient lists, we requested double the number of our target sample size (n=40). Our team then contacted patients through phone or email to set up interviews. Eligibility criteria included that the participant had spinal pain, could speak English, and were over 18 years of age. There were no eligibility criteria related to chronicity.
The qualitative phone interviews were semi-structured. Four members of our research team (MW, LH, PI and CG) conducted qualitative interviews. All of the interviewers were master’s degree-trained health services researchers with formal training in qualitative research methods – three female, one male. Participants were verbally consented at the start of the interview. The consent script explained that the research team sought to understand patients’ experiences with pain and with chiropractic care. Interviewers did not have any relationship with study participants prior to the study.
Participants were asked to describe their pain condition chronologically (narrative approach), including the duration of their pain condition and how their pain had changed over time.
We asked, “Do you consider this a chronic problem?” and “What do you consider to be a chronic [low back/neck] problem?” Patients were also asked to “give an overview of what you have done for your pain,” in particular the types of health care providers they had seen and what they liked and disliked about that care.
We also asked, “What did you hope to achieve with this treatment/provider?” They were asked basic sociodemographic questions such as age, sex, income, educational attainment, and race/ethnicity.
The interviews were conducted by four health policy researchers and lasted 30–45 minutes each. The team audio-recorded the interviews and took detailed notes throughout. Participants received a $30 electronic gift card as an incentive for study participation. Qualitative phone interviews were conducted from late 2014 to early 2015.
Qualitative analysis was conducted by the same four team members who conducted the phone interviews, with supervision from a senior researcher with extensive qualitative research experience. The team agreed to conclude interviews when they thought they had reached data saturation, which for this study meant that the range of patient experiences with spinal pain had been adequately represented across the qualitative data.
The research team reviewed the responses to each interview question and treated them as free list (i.e., open-ended, unstructured and unordered responses). To identify salient subthemes, the team used an inductive pile-sorting technique described by Lincoln and Guba [43] and further elaborated by Ryan and Bernard. [44]
The team printed each item from a single question on a separate piece of paper, noting the interview ID number on the back. Pieces of paper were spread over a large table, and team members as a group sorted the items into piles based on their similarities.
Once the team reached consensus on which items belonged in which pile, the piles were named and recorded. Each pile would represent a single thematic category, and those categories could be further sorted into subcategories – for instance, a pile that focused on coping approaches could be separated into specific approaches used for coping.
Study 2 qualitative pilot survey items:
The research team recruited pilot survey participants from the same five Los Angeles-area chiropractic clinics described above. The pilot survey took place after all the study 1 exploratory interviews were complete. This activity is referred to as a “pilot” survey because the team was pilot testing the recruitment and data collection methods that would later be used in the national survey, described below.
To recruit participants, the research team provided clinics with a web-enabled tablet that was pre-programmed with an online recruitment form. Clinic staff were instructed to ask all patients who entered the clinic during a one-month period to complete the pilot study recruitment form. Patients who met the study criteria were invited to continue completing an online consent form and surveys over the next three months.
Inclusion criteria for the pilot study included having low back and/or neck pain. There were also a number of exclusion criteria, because participants in the pilot study were also invited to participate in additional study components involving review of their health records and assessment of appropriateness of care. [34]
Exclusion criteria included age under 21 years, being unable to complete surveys in English, having an active workers compensation claim (because of potential differences in treatment and documentation) and having pain that was caused by certain specific medical conditions including cancer, pregnancy, fibromyalgia, and rheumatoid arthritis. We did not have exclusion criteria based on participation in the study 1 exploratory phone interviews, so the same patients could have participated in both studies.
The pilot study was a longitudinal study wherein participants completed up to 8 different surveys over a 3-month-period. The findings presented in this paper are all from the baseline survey. The pilot survey included a mix of qualitative and quantitative items that assessed the characteristics of the patients’ pain condition, their attitudes and beliefs about their condition, and experiences with treatment and coping.
The selection of items for the study 2 pilot survey was informed by the study 1 exploratory phone interviews. Qualitative questions included for analysis here were similar to the questions described above from the qualitative phone interviews. For instance, participants were asked to reflect generally on the meaning of chronicity: “People have different ideas about what it means for pain to be chronic. What does chronic pain mean to you?”
Patients were then asked to assess their own condition: “You stated that you consider your [low back/neck] pain to be chronic/not chronic. Why do you think so?” They typed their responses into a free-response field in the web survey. Pilot study participants were asked the same sociodemographic questions as the phone interview participants. Participants received up to $200 in electronic gift cards for completing all 8 pilot surveys. The pilot survey was conducted in 2015.
For this analysis, the qualitative pilot data responses were treated as additional observations alongside the existing qualitative phone interview data. The new data was analyzed using the same thematic pile sorting approach described above. In this paper, we report general demographic characteristics for both samples and key themes and narratives that were identified.
National survey
Within our sequential mixed methods design, qualitative data informed the development of the national survey through building our understanding of how patients’ understood core concepts related to pain and shaping our understanding of priority topics, from a patient perspective, that needed to be captured in the data collection. [42] This foreground qualitative research was used to refine the eligibility criteria for the national survey, and shaped follow-up activities including health record review and expert panels about appropriate care.
We recruited 2,024 patients from 125 doctor of chiropractic practices from six US states: California, Florida, Minnesota, New York, Oregon, and Texas. Patients were recruited from each clinic over a 4-week period using the same web-based tablet method used in the pilot study.
Inclusion criteria included having chronic low back and/or chronic neck pain; Survey items were primarily quantitative in nature, with multiple choice responses. The methods of the national survey were informed in numerous ways by the earlier qualitative data collection; we describe those details below. The national survey was conducted in 2016 and 2017. A full explanation of the national study methods has been published elsewhere. [34, 45]
Results
Qualitative studies: Descriptive statistics, narratives and themes, and conceptual model

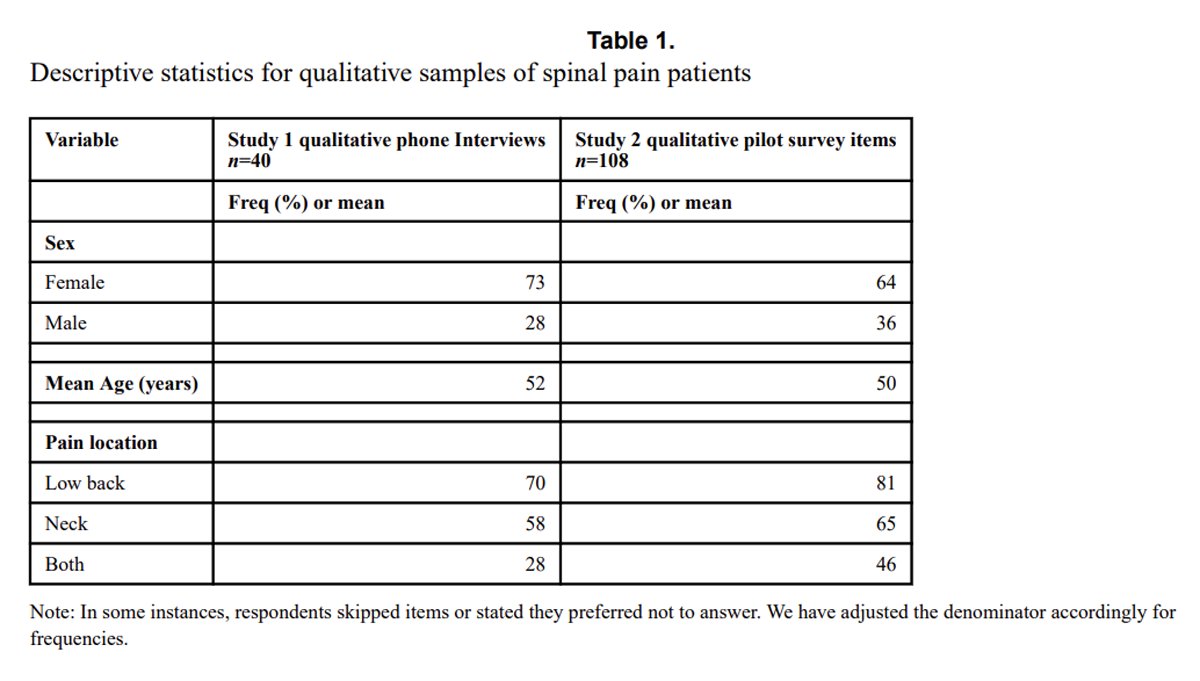
Table 1 We collected qualitative data about experiences with pain from n=148 chiropractic patients with spinal pain; n=40 underwent the exploratory qualitative phone interview, and n=108 underwent the qualitative pilot survey items. Sample characteristics are shown in Table 1, and a full set of sociodemographic characteristics are shown in the Appendix, Supplemental Table 1. Overall, the samples were predominately female with a mean age around 50 years. Regarding location of pain, over two-thirds of both samples had low back pain, and over half had neck pain.
Divergent pain narratives:
We identified two distinct narratives that patients used to describe their pain conditions: an acute pain narrative and a chronic pain narrative. Approximately three-quarters of interview participants fell into one of these two narratives; the remaining quarter had responses that did not fit clearly into either category.
In the acute narrative, conveyed by roughly one quarter of our participants, patients did not consider the pain to be chronic and still hoped to achieve a permanent cure for their pain. One example is a 60-year-old female patient who had back and neck pain for five months. She did not consider her pain to be chronic, which she defined as “something that you would have on a consistent basis for a long period of time, that you might expect to live with for a number of years.” Her expectation for her chiropractic treatment was to “eliminate the back and neck pain.” Similarly, a 47-year-old male patient had experienced low back pain on and off for nearly 20 years yet did not consider his pain chronic. He defined chronic pain as “always there, always present, never gone.” His expectation was that chiropractic treatment would make his pain go away permanently.
In contrast, roughly half of our respondents adhered to what we are describing as a chronic pain narrative, in which they did not expect a cure. They instead sought care hoping to reduce pain and/or to avoid flare ups. For example, a 25-year old male patient who had low back pain for 3 years considered his condition to be chronic, which he defined as pain that “is there everyday and it won’t go away or can’t be cured.” His goal for chiropractic care was to “decrease the pain.” Similarly, another patient, a 39-year-old woman, had been experiencing low back pain for 6 years and also considered her pain to be chronic, which she defined as “pain [that] doesn’t go away and has to be managed.” Her goal for chiropractic treatment was to “manage my pain.”
Chronicity as a constant presence:
When we asked participants in our qualitative studies what “chronic pain” meant to them, the majority described a condition that would always be present in their lives to some degree. “It means that it’s there, pretty much all the time and it will never go away” (54-year-old female patient, low back and neck pain for 14 years). Some observed that a person with chronic pain could have long periods with very little pain or even no pain at all, but the pain would eventually reappear. “It goes, but never forever. It creeps up and then creeps away” (60-year-old female patient, low back pain for 10 years).
Closely related to the idea that chronic pain “always comes back” (40-year-old female, neck pain, 5 years), was the belief that chronic pain is unlikely to ever resolve completely. One male patient (41 years of age) with low back and neck pain for 1 year said, “To me, chronic means that it…cannot be cured.” Some patients described negative feelings about having a chronic, permanent health problem, saying that having pain that never goes away “wears you down mentally and physically” (59-year-old male, low back and neck pain, 5 years) Others, like a 54-year-old female patient who had had low back and neck pain for 3 months, had accepted her condition, noting that she “managed pain and continue living. It’s there and it’s OK.” Patients described how this kind of chronic pain impacted their life. One female patient (age 51 years) who had had low back pain for 3 years mentioned how unexpected recurrences of pain would sometimes ruin her plans, as happened when she had to cancel plans to go to an amusement park. “You can’t plan since you never know.”
Commitment to long term management rather than cure-seeking:
Some patients expressed that while they would ideally like their pain to be cured, they had concluded that this was impossible. One female patient (age 54 years) with low back and neck pain for over 10 years, in discussing whether providers could reduce her pain completely, stated “no one has said they could bring it to zero, at any price.” Another, a female patient (age 55 years) with neck pain for 10 years, similarly observed, “No doctor can guarantee it will go away.” About her experience with chiropractic care, a 66-year-old female patient who had had low back and neck pain for less than a week, noted, “it’s not going to cure me.”
Others commented that a cure might be possible, but only with drastic measures that they did not want to undergo. A 68-year-old male patient who had had neck pain for 3 to 6 months stated, “You can’t get permanent relief unless you attempt surgery and I’m not planning to.” Instead, patients committed to ongoing management. Many reported that they liked chiropractic care because, even if it was not going to cure their condition, it helped them maintain function and avoid invasive treatments. A 51-year-old female patient who had experienced low back pain for 3 years noted that chiropractic care “doesn’t involve surgery, and it doesn’t involve drugs, and it allows me to maintain movement and normalcy as possible.”
It was important to patients to take action to avoid the pain flaring up. A 54-year-old male patient who had neck pain for 8 years observed, “You know for certain it will happen in the future if nothing is done to manage it.” Further, patients described how, over time, they had learned how to respond to their pain. A 70-year-old female patient who had experienced low back pain for 2 years said she felt empowered by the stretches that her chiropractor had taught her: “I am able to recognize the ache and then regardless of where I am… I can stop and do a stretch.” She added, “it’s always there. And if I didn’t do daily maintenance, I would have pain.”
Many patients described keeping a regular schedule of maintenance care, or “tune-up” visits, to prevent pain from flaring up. One female patient (age 68 years) with low back pain for two years explained it saying, “I have a standing appointment every two weeks. If I’m on vacation, and I miss the two-week appointment, the pain comes back… It’s incredible how maintenance helps.” A male patient (age 70 years) with low back pain for 6 years stated that his goal with chiropractic care was “to help maintain and keep it [pain] under control to where it’s the least amount of pain; it’s a chronic issue, so [I want to] keep my body adjusted and aligned so I’m least affected by it.”
Using a conceptual framework to inform quantitative studies:
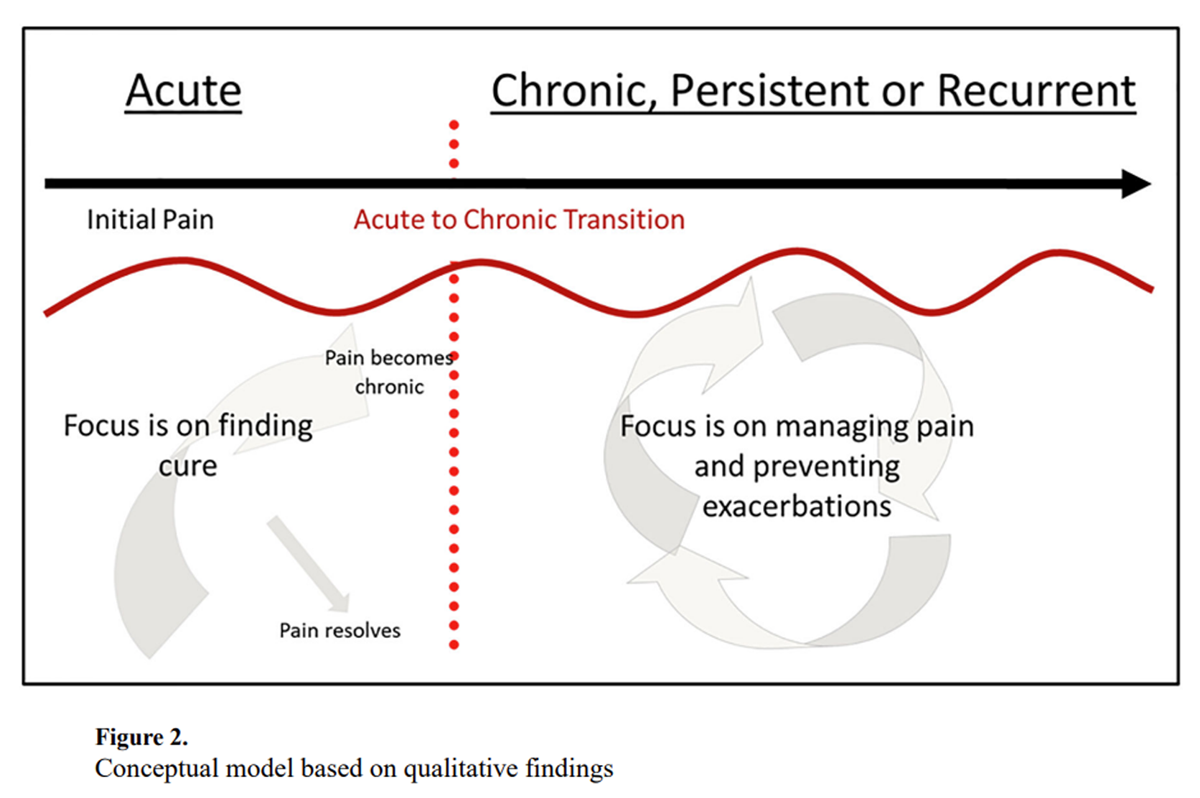
Figure 2 The research team organized the findings from the qualitative studies into a conceptual framework, shown in Figure 2. The framework shows, on the left-hand side, an acute phase of the pain condition wherein the patients’ focus is on finding a cure. For some patients, the pain condition resolves during this stage. For others, it becomes a chronic condition. The red dotted line represents the transition from an acute to a chronic narrative or conceptualization of their condition. In the chronic phase, the patient believes their condition will continue indefinitely, and their focus is on managing pain and preventing exacerbations.
This framework guided the research team in translating the qualitative findings into new quantitative items for the national survey, including the new item described below about treatment expectations. It helped ensure that the team shared an understanding of the key concepts and their interrelationships. Notably, our team developed this framework starting in 2015; more recently, major biomedical research endeavors like the Acute to Chronic Pain Signatures program have begun to explore related topics in much greater depth. [46, 47]
National study: Inclusion criteria and instrument informed by initial qualitative research
The research team conducted a US-wide study about experiences, beliefs and outcomes among chiropractic patients with chronic low back and neck pain. The focus specifically on chronic pain was distinct from the initial qualitative work, which included patients whose pain was not chronic. A methodological challenge in the design of the national survey was determining which definition of chronicity to apply for our inclusion criteria. The National Institutes of Health Task Force on Research Standards for Chronic Low Back Pain defines chronic low back pain as duration of at least three months, with pain for at least half the days over 6 months. [7]
At the same time, qualitative studies demonstrated that many participants defined chronicity not in terms of duration but instead as a condition that will always be present and requires long term management. So, there could have been patients who considered their condition chronic, but did not meet the Task Force definition, and vice versa. [48] The research team wanted the national study to respect both definitions and to recruit a sufficiently broad and diverse group of patients from each clinic. For this reason, we decided that our national study’s inclusion criteria would include patients if they perceived their condition to be chronic and/or if they had pain for at least 3 months. Specifically, they answered “Yes” or “I don’t know” to the question, “do you think your [low back or neck] pain is chronic?” or they gave a response equal or greater to 90 days to the question “How long did you have [low back or neck] pain before seeing a chiropractor?”
Informed by the qualitative findings that many spinal pain patients did not expect or seek a permanent cure to their pain condition and guided by our conceptual framework (Figure 2), the team created a multiple-choice survey item to collect quantitative survey data about these beliefs and expectations (Figure 1). Separate items were administered for low back pain and for neck pain; respondents with both types of pain responded to both items. The items were pre-tested in cognitive interviews and time tests and then administered in the national surveys.
Applying the new inclusion criteria and survey item, we found that among those with chronic low back pain, 32% had a goal for the pain to be cured permanently, while 31% sought to ease their pain or make it temporarily go away, 22% sought to prevent pain from coming back, and 14% sought to prevent pain from getting worse. Multivariate modeling showed that treatment goals varied based on participants’ attitudes about pain and the characteristics of their pain condition. For instance, participants who had experienced pain for a shorter period of time were more likely to hope for a permanent cure, while those with other treatment expectations had typically experienced pain for longer.
Discussion
This Center of Excellence for Research on CIH provided an opportunity to examine the many ways that formative qualitative research shape quantitative efforts and later studies that build on it. [34] Open-ended qualitative data collection led to insights that challenged the research team’s assumption that chronicity is only understood in terms of either pain duration or intensity, and rather that patients experience significant shifts in their relationship to their pain and in how they perceive the potential for pain management.
These insights informed not only a quantitative study and expert panel, but also various additional research activities and secondary studies that built on our national quantitative data collection. For instance, the Center convened two sets of expert appropriateness panels about spinal manipulative therapy and mobilization for chronic low back pain [49, 50] and for chronic neck pain, [51, 52] wherein panelists rated the appropriateness of spinal manipulative therapy and mobilization for distinct clinical scenarios.
In two panels, panelists were presented with the Center’s full conceptual framework and findings from the national study; many panelists observed that their appropriateness ratings could be changed based on patient preferences. [37] This work was cited in a subsequent modified delphi study about spinal manipulative therapy [53] and in published guidelines about epidural interventions for chronic spinal pain. [54] In addition, the national study data served as secondary data to answer research questions about topics including socioeconomic disparities in pain self-efficacy [55] and sleep disturbance among chronic pain patients. [56]
We applied a mixed methods approach at the study design level, specifically an exploratory-sequential design, [42] and in this work we describe both the qualitative and quantitative findings. Prior research had applied qualitative methods [57] or quantitative methods [58, 59] to understand what chiropractic patients expect from their care, underscoring, for instance, that most patients expect a reduction in pain and an explanation for their condition; [58, 59] however, mixed methods has been less common in this area.
MacPherson and colleagues, for example, used qualitative research to develop a full scale quantitative study of chiropractic patients in the United Kingdom, [59] but their qualitative results were not published. Jensen and colleagues studied expectations among Danish patients seeking chiropractic care for lumbar radiculopathy; their approach of using first quantitative then qualitative methods offered insight into the survey results, like the fact that high satisfaction ratings with chiropractic due were due in part to patients’ appreciation of the thorough examination and consultation provided by the chiropractors. [33] While informative, this was distinct from our team’s approach of asking patients in an open-ended fashion about their expectations, and then using that to design a full scale national survey.
Our findings align with earlier work as well. In our national survey, we found that two-thirds of chiropractic patients with chronic low back pain sought to ease their pain temporarily or prevent it from coming back or getting worse, while one third sought a permanent cure. Earlier work identified that many new chiropractic patients do anticipate a cure, while some proportion – albeit far smaller than what we observed – do not anticipate a cure to their pain.
In Sigrell’s 2002 quantitative survey of new chiropractic patients in Sweden, two-thirds of patients expected to be “symptom free” after their treatment, while one quarter were uncertain and about 7% did not expect this. [58]
Sigrell attributed some of these neutral or negative expectations to a perception among some patients that chiropractic care was a last resort after other treatments had failed. In a 2015 qualitative study of U.S. low back pain patients who tried multiple forms of CIH care, including chiropractic, Eaves and colleagues observed that over time, some patients focused less on cure-seeking and more on long-term management of their condition; this aligns closely with our qualitative findings about expectations for outcomes among ongoing chiropractic patients. [60, 61]
Shannon and colleagues’ 2018 study showed that patients and other stakeholders in a rural U.S. rehabilitation hospital expected chiropractic care to support pain relief, function, ongoing management, and overall healthy living. [57] Lastly, our team’s qualitative findings about how patients may shift focus toward managing their chronic pain rather than eliminating their pain builds on other scholarship about the transition from acute pain to chronic pain research. [62, 63]
What our qualitative study participants described in terms of adopting a chronic pain mentality and focusing on managing their conditions may be related to the goals of psychological pain therapies, such as Acceptance and Commitment Therapy and Mindfulness-Based Cognitive Therapy, which focuses on enhancing flexibility and taking concrete steps toward meaningful living even in the midst of mental and physical health challenges. [64–67] They also relate to the goals of pain education programs, which typically aim to help patients understand the physiology of pain, psychosocial elements of pain and the importance of being physically active. [68–70] Our findings also align with recommendations to adopt pain management programs that focus on improving functioning and quality of life for patients who continue experiencing pain after trying other evidence-based treatments. [13]
The findings also connect with the growing literature about patient-centered care broadly and in the area of pain. [71] The Veterans Affairs’ Whole Health model similarly encourages a patient-centered perspective. [72, 73]
Sullivan describes the need to move toward a fuller understanding of the salience of pain in a patient’s life when considering which therapies are most appropriate. [11] Shared understandings between patients and providers and respect for patient’s preferences are core components of patient-centered care, which is now a guiding aim of healthcare in the US and elsewhere. [74] Research on patients’ understandings of their conditions and preferences for care are necessary to accomplish patient-centered care. Incorporating qualitative insights from patients ensures that quantitative tools used to assess pain are rooted in the actual experiences of those patients.
Strengths and limitations
This study collected data only from chiropractic patients. Roughly half of Americans have seen a chiropractor, [25] and our study provides new information about the types of patients who seek nonpharmacological treatments for pain and how they relate to their condition. [75] Spinal manipulative therapy, which is typically provided by chiropractors, features importantly along with other CIH care among evidence-based alternatives to opioid pain treatments; other options include meditation, acupuncture, massage therapy, physical therapy, and other non-pharmacological interventions. [12, 19] However, an important limitation of this work is that the findings may not generalize to the patient populations of other healthcare modalities.
In addition, the qualitative data described here were collected 10 years ago. We do not believe that people’s understandings of chronicity would have changed since then, although there may now be more openness to CIH treatments for back pain and potentially more insurance coverage for CIH treatments such as chiropractic care. [76]
Attitudes toward healthcare may have evolved during this time in response to the COVID-19 pandemic and societal changes. [77, 78] In addition, the prevalence of spinal pain increased by two percentage points during the course of the COVID-19 pandemic, in parallel with increases in other types of pain. [79] While our qualitative data were collected well before the pandemic, it is a unique advantage to be able to retrospectively examine how those findings were integrated into later stages of research.
Our study had methodological limitations as well. In the qualitative interviews, three-quarters of participants fit into one of the two pain condition narratives, while one quarter did not, because their answers did not clearly fit into either narrative. In some cases, it was because the answers were brief and offered little detail. It is possible that with more intentional probing or targeted questioning, we could have categorized the remaining quarter of individuals. Further, there were strengths and challenges that arose from applying both qualitative and quantitative methods within a study. While it enabled a more comprehensive understanding of the phenomena of chronic pain, it also required bringing together two differing sets of epistemological assumptions and analytic approaches. It was challenging to align the findings across both components and ensure coherence across data sources. Additionally, the relatively smaller, context-specific qualitative sample may limit generalizability and complicate direct comparison or integration with quantitatively-derived results.
Conclusion
Using an exploratory sequential mixed methods design to capture data about chiropractic patients’ preferences, experiences, and beliefs about spinal pain, [42] we developed a framework that describes a shift in the approach to treatment for spinal pain patients at different stages of their pain condition (i.e., acute vs. chronic).
Initial qualitative research revealed that many patients defined chronicity not in terms of intensity or time-bound duration, but rather in regards to its permanence (i.e., as a condition that would always be present). Many patients with chronic pain did not expect to obtain a cure for their condition but instead were committed to long-term management of their condition.
These findings shaped the inclusion criteria and instrument for a national survey of over 2,000 chronic pain patients, in which we found that less than a third of spinal pain patients in the sample expected that their pain could be cured, while the majority sought to either ease pain or make it go away temporarily, or to prevent it from returning or worsening. [37]
This work can inform future research and practice in two distinct ways. First, the finding that many spinal pain patients in this sample viewed chronic pain as permanent may have implications for other studies, especially inclusion criteria. Defining chronicity only in terms of duration, frequency, or intensity may leave out patients who define their pain in terms of its permanence or lack thereof.
For a patient-centered approach, researchers should consider simply asking patients if they consider their pain to be chronic as well as what that might mean to them. Second, this paper provides a useful example of an exploratory sequential mixed methods approach for building national surveys.
Effective approaches used in this Center included its multidisciplinary team of researchers and the use of a visual framework to capture, communicate, and refine the qualitative findings with a large team.
Supplementary Material
Appendix - Supplemental Table 1
Supplemental Table 1. Sociodemographic characteristics of study participants (16.5KB, docx)
Funding sources:
Research reported in this publication was supported by the National Center for Complementary & Integrative Health of the National Institutes of Health under Award Numbers U19AT007912 and U24AT012549.
RSW receives funding from the grant K12NS130673 from the National Institute of Neurological Disorders and Stroke.
The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health, the National Center for Complementary and Integrative Health, or the National Institute of Neurological Disorders and Stroke.
Abbreviations
CIH = complementary and integrative healthcare
DC = Doctor of chiropractic
NIH = National Institutes of Health
Declaration of generative AI and AI-assisted technologies in the writing process:
The research team did not use generative AI to write the manuscript text nor to edit it; AI was also not used to conduct data analysis. The lead author used an AI-assisted literature review program called Perplexity AI to search for relevant literature and identify a small number of the references included in the paper; the author read through any identified articles to determine their relevance to the paper.
References
Ferreira ML, de Luca K, Haile LM, et al.
Global, Regional, and National Burden of Low Back Pain,
1990–2020, Its Attributable Risk Factors, and
Projections to 2050: A Systematic Analysis of
the Global Burden of Disease Study 2021
Lancet Rheumatology 2023 (May 23); 5 (6): E316-E329Hoy D, March L, Woolf A, et al. ,
The Global Burden of Neck Pain:
Estimates From the Global Burden of Disease 2010 Study
Ann Rheum Dis. 2014 (Jul); 73 (7): 1309–1315 .Hoy D, March L, Brooks P, et al.
The Global Burden of Low Back Pain:
Estimates from the Global Burden of Disease 2010 study
Ann Rheum Dis. 2014 (Jun); 73 (6): 968–974Martin BI, Deyo RA, Mirza SK, et al.
Expenditures and health status among adults with back and neck problems
Jama 299 (2008) 656–64.Fenske J, Berland D, Chandran S, et al.
Pain Management
Ann Arbor (MI)2021. [Available from:
https://www.ncbi.nlm.nih.gov/books/NBK572296/National Institute of Neurological Disorders and Stroke.
Pain 2025
[cited 2025 April 18]. Available from:
https://www.ninds.nih.gov/health-information/disorders/painDeyo RA, Dworkin SF, Amtmann D, et al.
Report of the NIH Task Force on Research
Standards for Chronic Low Back Pain
Journal of Pain 2014 (Jun); 15 (6): 569–585Treede RD, Rief W, Barke A, et al.
Chronic pain as a symptom or a disease: the IASP Classification of Chronic Pain for the International Classification of Diseases (ICD-11)
Pain 160 (2019) 19–27.Kosek E, Clauw D, Nijs J, et al.
Chronic nociplastic pain affecting the musculoskeletal system: clinical criteria and grading system
Pain 162 (2021) 2629–34
SEE THIS:: Nociplastic Pain: An Introduction
J Can Chiropr Assoc 2025 (Aug); 69 (2): 131–144Fitzcharles M-A, Cohen SP, Clauw DJ, et al.
Nociplastic pain: towards an understanding of prevalent pain conditions
The Lancet 397 (2021) 2098–110.Sullivan MD
What do we owe patients with chronic pain?
Pain Med 20 (2019) 878–81.Joint Commission
Non-Pharmacologic and Non-Opioid Solutions for Pain Management
2018. Aug 2018Gauntlett-Gilbert J, Brook P
Living well with chronic pain: the role of pain-management programmes
BJA Education 18 (2018) 3–7.Board on Health Sciences Policy Committee on
Advancing Pain Research Care
Relieving Pain in America: A Blueprint for Transforming
Prevention, Care, Education, and Research
National Academies Press; 2011.Driscoll MA, Knobf MT, Higgins DM, et al.
Patient experiences navigating chronic pain management in an integrated health care system: A qualitative investigation of women and men
Pain Medicine 19 (2018) S19–S29.
SEE THIS:: A Supermarket Approach to the Evidence-informed
Management of Chronic Low Back Pain
Spine J. 2008 (Jan); 8 (1): 1–7Cashin AG, Furlong BM, Kamper SJ, et al.
Analgesic effects of non-surgical and non-interventional treatments for low back pain: a systematic review and meta-analysis of placebo-controlled randomised trials
BMJ Evid Based Med (2025) bmjebm–2024–112974.Corp N, Mansell G, Stynes S, et al.
Evidence-based treatment recommendations for neck and low back pain across Europe: A systematic review of guidelines
Eur J Pain 25 (2021) 275–95.National Center for Complementary and Integrative Health (NCCIH)
Pain: Considering Complementary Approaches 2023
15 chapters; 52 pagesHerman PM, Maiers MJ, Burdick RR, et al.
Alternatives to Opioids: A Missing Piece of the Strategy
Santa Monica, CA: RAND Corporation; (Aug 29, 2023) 20 pages.Rodrigues dos Santos BM, Mendes C
Manual therapy and its role in occupational health: Reducing absenteeism and presenteeism by treating chronic pain with spinal manipulation and mobilization in the workplace
Eur J Integr Med 35 (2020) 101078.Leach MJ, Climstein M, Fryer G, et al.
Developing a needs-based integrative service delivery model to deliver best practice care for chronic nonspecific low back pain
Eur J Integr Med 53 (2022) 102153.Herman PM, Coulter ID
Complementary and Alternative Medicine: Professions or Modalities?
Policy Implications for Coverage, Licensure, Scope of
Practice, Institutional Privileges, and Research
RAND Corporation; 2015Barnes PM, Bloom B, Nahin RL,
Complementary and Alternative Medicine Use Among
Adults and Children: United States, 2007
Natl Health Stat Report Number 12 December 10, 2008 (2015) 1–16.Clarke TC, Black LI, Stussman BJ, et al.
Trends in the Use of Complementary Health Approaches
Among Adults: United States, 2002–2012
Natl Health Stat Report Number 79 February 10, 2015English C, Keating E
Majority in U.S. say chiropractic works for neck, back pain
Gallup; 2015Sirois FM
Treatment seeking and experience with complementary/alternative medicine: A continuum of choice
J Altern Complement Med 8 (2002) 127–34Thomas KJ, Nicholl JP, Fall M
Access to complementary medicine via general practice
Br J Gen Pract 51 (2001) 25–30.Penney LS, Ritenbaugh C, Elder C, et al.
Primary care physicians, acupuncture and chiropractic clinicians, and chronic pain patients: a qualitative analysis of communication and care coordination patterns
BMC Complementary and Alternative Medicine 16 (2016) 30.Benson M, Albanese A, Bhatia KP, et al.
Development of a patient journey map for people living with cervical dystonia
Orphanet Journal of Rare Diseases 17 (2022) 130.Ayers SL, Kronenfeld JJ
Delays in seeking conventional medical care and complementary and alternative medicine utilization
Health Services Research 47 (2012) 2081–96.Bishop FL, Yardley L, Lewith GT
Why consumers maintain complementary and alternative medicine use: A qualitative study
J Altern Complement Med 16 (2010) 175–82O’Cathain A, Murphy E, Nicholl J
The quality of mixed methods studies in health services research
J Health Serv Res Policy 13 (2008) 92–8Jensen RK, Lillesř S, Jensen JS, et al.
Patient Expectations and Levels of Satisfaction in
Chiropractic Treatment for Lumbar Radiculopathy.
A Mixed Methods Study
Chiropractic & Manual Therapies 2023 (May 19); 31: 13Coulter ID, Herman PM, Ryan GW, et al.
Researching the Appropriateness of Care in the Complementary
and Integrative Health Professions: Part I
J Manipulative Physiol Ther. 2018 (Nov); 41 (9): 800–806World Health Organization. Regional Office for Europe.
Appropriateness in health care services: Report on a WHO workshop
Koblenz, Germany, 23–25 March 2000. Copenhagen: 2000.
[Available from: https://apps.who.int/iris/handle/10665/108350Rubinstein SM, de Zoete A, van Middelkoop M, et al.
Benefits and Harms of Spinal Manipulative Therapy for the
Treatment of Chronic Low Back Pain: Systematic Review
and Meta-analysis of Randomised Controlled Trials
British Medical Journal 2019 (Mar 13); 364: 1689Herman PM, Whitley MD, Ryan GW, et al.
The impact of patient preferences and costs on the appropriateness of spinal manipulation and mobilization for chronic low back pain and chronic neck pain
BMC Musculoskelet Disord 20 (2019) 1–10Whitley MD, Coulter ID, Gery RW, et al.
Researching the Appropriateness of Care in the
Complementary and Integrative Health Professions:
Part 3: Designing Instruments With Patient Input
J Manipulative Physiol Ther. 2019 (Jun); 42 (5): 307–318Sherbourne CD, Ryan GW, Whitley MD, et al.
Coping and management techniques used by chronic low back pain patients receiving treatment from chiropractors
J Manipulative Physiol Ther 42 (2019) 582–93.Herman PM, Luoto JE, Kommareddi M, et al.
Patient Willingness to Pay for Reductions in Chronic
Low Back Pain and Chronic Neck Pain
J Pain 2019 (Nov); 20 (11): 1317–1327Hays RD, Sherbourne CD, Spritzer KL, et al.
Experiences with Chiropractic Care for
Patients With Low Back or Neck Pain
J Patient Exp 2020 (Jun); 7 (3): 357–364Fetters MD, Curry LA, Creswell JW
Achieving integration in mixed methods designs—principles and practices
Health Serv Res 48 (2013) 2134–56.Lincoln YS, Guba EG
Naturalistic Inquiry.
Beverly Hills, CA: Sage; 1985.Ryan GW, Bernard HR
Techniques to Identify Themes
Field Methods 15 (2003) 85–109.Herman PM, Kommareddi M, Sorbero ME, et al.
Characteristics of Chiropractic Patients Being Treated
for Chronic Low Back and Neck Pain
J Manipulative Physiol Ther. 2018 (Jul); 41 (6): 445–455Wager TD, Sutherland SP, Lindquist MA, et al.
Accelerating discovery in pain science: the Acute to Chronic Pain Signatures program
Pain 166 (2025)The University of Texas at Austin.
Acute to Chronic Pain Signatures 2021.
[Available from: https://a2cps.org/Hilton LG, Whitley MD, Gery RW, et al.
Differing definitions of chronic pain: Comparison of patients, providers, and researchers from a national clinical sample.
American Public Health Association Annual Meeting and Expo;
Nov 10–14, 2018; San Diego, CA: 2018.Coulter ID, Whitley MD, Hurwitz E, et al.
Determining the Appropriateness of Spinal Manipulation and Mobilization for Chronic Low Back Pain: Indications and Ratings by a Multidisciplinary Expert Panel
Santa Monica, CA: RAND Corporation; 2018.Herman PM, Hurwitz EL, Shekelle PG, et al.
Clinical scenarios for which spinal mobilization and manipulation are considered by an expert panel to be inappropriate (and appropriate) for patients with chronic low back pain
Clin J Pain 2020 (Apr); 36 (4): 273–280Coulter ID, Whitley MD, Vernon H, et al.
Determining the Appropriateness of Spinal Manipulation
and Mobilization for Chronic Neck Pain: Indications
and Ratings by a Multidisciplinary Expert Panel
Santa Monica, CA: RAND Corporation; 2018Herman PM, Vernon H, Hurwitz EL, et al.
Clinical Scenarios for Which Cervical Mobilization and
Manipulation Are Considered by an Expert Panel to
Be Appropriate (and Inappropriate) for Patients
with Chronic Neck Pain
Clin J Pain 2020 (Apr); 36 (4): 273–280Innes S, Beynon A, Hodgetts C, et al.
Predictors of instantaneous relief from spinal manipulation for non-specific low back pain: a delphi study
Chiropr Man Therap 28 (2020) 39Manchikanti L, Knezevic NN, Navani A, et al.
Epidural interventions in the management of chronic spinal pain: American Society of Interventional Pain Physicians (ASIPP) comprehensive evidence-based guidelines
Pain Physician 24 (2021) 27Whitley MD, Herman PM, Aliyev GR, et al.
Income as a predictor of self-efficacy for managing pain and for coping with symptoms among patients with chronic low back pain
J Manipulative Physiol Ther 44 (2021) 433–44Qureshi N, Siconolfi D, Rodriguez A, et al.
Comparing three measures of sleep disturbance in persons with chronic low back and neck pain
Adv Patient-Rep Outcomes (2025) 100187Shannon ZK, Salsbury SA, Gosselin D, et al.
Stakeholder Expectations from the Integration of Chiropractic
Care into a Rehabilitation Setting: A Qualitative Study
BMC Complementary Alternative Medicine 2018 (Dec 4); 18 (1): 316Sigrell H
Expectations of chiropractic treatment: what are the expectations of new patients consulting a chiropractor, and do chiropractors and patients have similar expectations?
J Manipulative Physiol Ther 25 (2002) 300–5MacPherson H, Newbronner E, Chamberlain R, et al.
Patients' Experiences and Expectations of Chiropractic Care:
A National Cross-sectional Survey
Chiropractic & Manual Therapies 2015 (Jan 16); 23 (1): 3Eaves ER, Sherman KJ, Ritenbaugh C, et al.
A Qualitative Study of Changes in Expectations Over Time
Among Patients with Chronic Low Back Pain
Seeking Four CAM Therapies
BMC Complement Altern Med. 2015 (Feb 5); 15: 12Hsu C, Sherman KJ, Eaves ER, et al.
New perspectives on patient expectations of treatment outcomes: results from qualitative interviews with patients seeking complementary and alternative medicine treatments for chronic low back pain
BMC Complement Altern Med 14 (2014) 276Cohen SP, Vase L, Hooten WM
Chronic pain: an update on burden, best practices, and new advances
Lancet 397 (2021) 2082–97.Chapman CR, Vierck CJ
The Transition of Acute Postoperative Pain to Chronic Pain: An Integrative Overview of Research on Mechanisms
J Pain 18 (2017) 359.e1–.e38.Allen KD, Ambrose KR, Booker SQ, et al.
Non-pharmacological pain management for osteoarthritis: review update
Curr Rheumatol Rep 27 (2025) 19.McCracken LM, Vowles KE
Acceptance and commitment therapy and mindfulness for chronic pain: model, process, and progress
Am Psychol 69 (2014) 178–87Hayes SC, Strosahl KD, Wilson KG
Acceptance and Commitment Therapy, Second Edition:
The Process and Practice of Mindful Change:
Guilford Publications; 2011.Alsubaie M, Abbott R, Dunn B, et al.
Mechanisms of action in mindfulness-based cognitive therapy (MBCT) and mindfulness-based stress reduction (MBSR) in people with physical and/or psychological conditions: A systematic review
Clinical psychology review 55 (2017) 74–91Saracoglu I, Arik MI, Afsar E, et al.
The short-term effects of neuroscience pain education on quality of life in patients with chronic low back pain: A single-blinded randomized controlled trial
Eur J Integr Med 33 (2020) 101046.Darnall BD, Roy A, Chen AL, et al.
Comparison of a single-session pain management skills intervention with a single-session health education intervention and 8 sessions of cognitive behavioral therapy in adults with chronic low back pain: A randomized clinical trial
JAMA Netw Open 4 (2021) e2113401–e.Ryan CG, Karran EL, Wallwork SB, et al.
We Are All in This Together-Whole of community pain science education campaigns to promote better management of persistent pain
J Pain 25 (2024) 902–17Centers for Medicare and Medicaid Services.
Chronic Pain Experience map no date [cited May 20 2025].
Available from: https://www.cms.gov/files/document/
cms-chronic-pain-journey-map.pdfBokhour BG, Haun JN, Hyde J, et al.
Transforming the Veterans Affairs to a Whole Health
System of Care: Time for Action and Research
Medical Care 2020 (Apr); 58 (4): 295–300National Academies of Sciences E., and Medicine
Achieving Whole Health: A New Approach for Veterans and the Nation.
Washington, DC; 2023Institute of Medicine Committee on Quality of Health Care in America.
Crossing the Quality Chasm:
A New Health System for the 21st Century
Washington (DC): National Academies Press (US); 2001Qaseem A, Wilt TJ, McLean RM, et al.
Noninvasive Treatments for Acute, Subacute, and Chronic
Low Back Pain: A Clinical Practice Guideline From
the American College of Physicians
Annals of Internal Medicine 2017 (Apr 4); 166 (7): 514–530Nahin RL, Barnes PM, Stussman BJ
Insurance Coverage for Complementary Health Approaches
Among Adult Users: United States, 2002 and 2012
NCHS Data Brief No. 235 January 2016
US Department of Health and Human Services,
Centers for Disease Control and Prevention,
National Center for Health StatisticsPark CL, Russell BS, Fendrich M, et al.
Americans’ COVID-19 stress, coping, and adherence to CDC guidelines
J Gen Intern Med 35 (2020) 2296–303Frieden TR, Rajkumar R, Mostashari F
We must fix US health and public health policy
Am J Public Health 111 (2021) 623–7Zajacova A, Grol-Prokopczyk H, Nahin RL
Pain among US adults before, during, and after the COVID-19 pandemic: a study using the 2019 to 2023 National Health Interview Survey
Pain (2025)
Return to SPINAL PAIN MANAGEMENT
Since 6-18-2026
| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |