

Where Are the Chiropractic
Clinical Outcomes Registries?
A Scoping ReviewThis section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: Chiropractic & Manual Therapies 2025 (May 25); 33: 22 ~ FULL TEXT
OPEN ACCESS Joel Carmichael • Kent Stuber • Katherine A Pohlman • Amy Ferguson • Michele Maiers
Department of Physical Medicine and Rehabilitation,
School of Medicine, University of Colorado Anschutz Medical Campus,
13121 E 17th Ave, Mail Stop C244,
Aurora, CO, 80045, USA.
You may also enjoy this self-review by the lead author. Objective: This scoping review maps chiropractic-specific clinical outcomes registries.
Introduction: Clinical outcomes registries track patient outcomes to improve evidence-based practice and quality of care; however, their role in chiropractic remains unclear.
Methods: This research adhered to Joanna Briggs Institute's scoping review outline and methodology, as well as the PRISMA-ScR guidelines. Five databases were searched on January 9, 2025, with subsequent search of grey literature and citation tracking. Sources were included if they described chiropractic-specific registries that reported clinical outcomes data. Two reviewers independently screened 604 citations, extracting data into Excel. Variables included registry characteristics and clinical outcomes collected.
Results: Only one dedicated chiropractic clinical outcomes registry was identified: Spine IQ, launched in 2016 in the US with approximately 50 chiropractors submitting data on over 2000 low back pain patients. Spine IQ collected patient-reported outcome measures including the Oswestry Disability Index, Bournemouth Questionnaire, and the PROMIS physical function measure. By 2018, Spine IQ had completed its pilot phase and planned expansion to 100 clinics. Three sources were excluded: one spine registry not collecting chiropractic outcomes and two databases that included chiropractic data in publications but did not qualify as registries.
Conclusions: This review identified only Spine IQ as a dedicated chiropractic clinical outcomes registry, revealing a significant gap in registry infrastructure within the profession globally. The profession should explore the development of registries to enhance care quality, societal impact, and opportunities for collaborative research.
Keywords: Chiropractic clinical outcomes; Patient-reported outcome measures; Registry.
From the FULL TEXT Article:
Introduction
A clinical registry is an organized data collection system used by clinicians [1, 2] to systematically gather clinical outcomes as data points over time from patients who share a specific health condition, intervention, or other characteristics. These clinical data points are relevant to changes in the health condition under study that may be associated with the intervention. [3] A registry’s primary purpose is to track trends in clinical outcomes, improve quality of care, benchmark healthcare performance, and support research and policymaking.
For the purposes of this scoping review, chiropractic clinical outcomes are defined as patient-reported clinical measures during or after chiropractic care, including patient symptoms and function. [4] These outcomes in a clinical registry are serially collected to gather data relevant to the condition or pathology under study.
For clarity, it is essential to distinguish clinical registries from clinical databases and Practice-based Research Networks (PBRNs). Clinical databases are broader and usually more comprehensive in scope whereas registries tend to be more focused and condition-specific. [5, 6] Clinical databases collect comprehensive patient data for more general purposes, such as patient billing and cost, administrative tasks, patient management (e.g., electronic health records), or ad hoc research. Data collection and the use of research in clinical databases are improvised or created as needed rather than being systematic or pre-planned, as is the case with clinical registries. Also, by contrast, PBRNs are organized collaborations of healthcare clinicians and practices that work together to answer healthcare questions, conduct research in everyday practice settings, and focus on care delivery and implementation science. [7] Unlike clinical registries, which use a standardized collection of clinical outcomes data for a pre-specified condition or set of conditions, PBRNs collect data for both prospective interventional trials and implementation research. While PBRNs may utilize clinical registry data collection modalities, they may also employ a broader range of data sources.
Rationale
Clinical outcomes data are fundamental to answering important research questions as they form the foundation of evidence-based practice [8], support quality improvement and patient safety initiatives [9, 10], enhance patient-centered care [11], facilitate regulatory approval [12], inform health policy [12], and advance research methodologies. [14]
Clinical registries amass large datasets that are cumulative over time, resulting in large sample sizes available for observational studies and pragmatic clinical research questions. By leveraging clinical outcomes data, clinicians and researchers can collaborate to enhance patient care and improve health outcomes. [15, 16]
When systematically collected and aggregated over the long term, clinical outcomes data in registries can provide powerful, actionable information with greater feasibility, cost-effectiveness, and longer-term follow-up compared to time-limited, often resource-intensive clinical trials [17], enabling clinicians to refine clinical care pathways, optimize treatment outcomes over the longer term, and personalize care for individual patients. [16] Over the past 30 years [2] such registries have also been used by clinicians, researchers, industry leaders, and policymakers to enhance patient care and quality of life [18], update clinical care guidelines, and inform healthcare policy. [19] The adoption of automated technologies, such as smartphones and portable computing devices, has facilitated the rapid expansion of clinical outcomes registries across various healthcare disciplines worldwide. [20–23] These advancements have yielded impactful clinical research derived from real-world healthcare settings. [20, 24, 25] When applied with proper analytic techniques, registry studies can approach the methodological rigor of randomized controlled trials. [26] Furthermore, registries serve as valuable resources for training researchers and clinical education. [27]
Chiropractic is a global profession with practitioners now established in over 90 countries across 6 continents. [28] As the profession continues to integrate into mainstream healthcare systems worldwide, the need for robust clinical evidence to inform best practices becomes increasingly important. Clinical outcomes registries may represent a valuable opportunity for the global chiropractic community to systematically document patient care and outcomes in diverse healthcare settings and cultural contexts.
Objective
Given the value of clinical registries in several key professional domains, knowledge of existing chiropractic registries is essential. The objective of this scoping review is to map chiropractic clinical outcomes registries worldwide.
Methods
Protocol and registration
This scoping review was guided by the Joanna Briggs Institute (JBI) Manual for Evidence Synthesis methodology [29] and the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews (PRISMA-ScR). [30]
The objectives, inclusion criteria, and methodology for this scoping review were developed in accordance with Peters et al. [31] and prospectively registered and published online with INPLASY on June 20, 2023 (10.37766/inplasy2023.6.0064). [32] This review did not require institutional review board (IRB) approval.
Eligibility criteriaTypes of participants
Eligible clinical registries for this review included those that described chiropractic patients of any age with any diagnosis, whose clinical outcomes data were collected and retained within the registry.
Concept
The core concept of this scoping review was to identify and map chiropractic-specific clinical registries reporting clinical outcomes collected in conjunction with chiropractic treatment encounters.
Context
This scoping review considered all clinical settings where clinical outcomes from chiropractic encounters were entered into a clinical registry.
Eligible information sources
Eligible clinical registries collected clinical outcomes data from patients receiving chiropractic care. Information sources included scientific journals, grey literature (e.g., chiropractic trade journals and magazines), conference proceedings, and clinical practice guidelines.
The search had no restrictions regarding socioeconomic status, healthcare system, location, demographics (including age, sex, gender, and race), military or civilian status, activity level, or insurance status of individuals whose data were collected by registries. Studies were excluded if they(1) did not meet registry definition criteria or
(2) lacked clinical outcomes data from patients receiving chiropractic care.
Search
A health sciences librarian collaborated with our research team to develop the search strategy and conduct a preliminary search. To ensure rigor and comprehensiveness, a second librarian independently applied the structured Peer Review of Electronic Search Strategies (PRESS) methodology. [33]
We refined our methods by:(1) establishing precise definitions and differentiating features between clinical outcomes registries and databases to ensure sources were limited to registries only,
(2) implementing citation tracking to identify additional registry reports, and
(3) expanding our scope beyond clinical journals to include grey literature.To ensure clarity in evidence source selection for this review we specified that “chiropractic clinical outcomes” excluded health service utilization, claims, survey, cost-effectiveness, and administrative data but did not exclude medication use. After these methodological refinements, the scoping review was conducted again in its entirety.
Medline (Ovid), CINAHL (EBSCO), Index to Chiropractic Literature (ICL), Alt HealthWatch (EBSCO), and SPORTDiscus (EBSCO) were searched on January 9, 2025. We performed citation tracking using CitationChaser. [34] All citations were retained in Covidence and exported to EndNote for use by the research team. The comprehensive search strings used in this scoping review appear in Appendix 1, Supplementary Materials.
Selection of sources of evidence
Citations were uploaded into EndNote 20 (Clarivate Analytics, PA, USA) and subsequently imported into Covidence (Veritas Health Innovation, Melbourne, Australia) for deduplication and screening. Two reviewers (KS and JC) conducted a pilot test of our initial title/abstract screening process for full-text review. They independently evaluated seven randomly selected abstracts to refine the process and ensure fidelity.
This pilot resulted in 100% agreement, exceeding the a priori threshold of 85% set by the authors. The two reviewers performed full-text evaluation to select articles for data extraction. Following selection, they conducted reference checking to identify additional potential evidence sources.
Disagreements between reviewers during full-text review were resolved through discussion and iterative refinement. A third reviewer from the study team was available for arbitration but not required. Similarly, after completing full-text reviews in Covidence independently, all disagreements regarding final article selection were resolved through discussion between the two reviewers.
Data charting process
This scoping review extracted data from full-text publications using a systematic manual approach rather than an automated selection tool. Data were organized in Excel and Word tables using predefined variables specific to chiropractic clinical registries that aligned with the objectives of this review. Supplementary information regarding registry characteristics was obtained through direct correspondence with registry owners and/or data managers.
Data items
Prespecified chiropractic registry variables extracted into Excel included each of the following: name and country of registry, date of registry inception together with years of operation and date of registry cessation, health conditions catalogued, treatment types and clinical outcomes tracked, and patient enrollment numbers for the registry. We also extracted the stated purpose of the registry, if any, and the status of the registry as of January 9, 2025.
Reporting of results
The broad scope and mapping objective of this review precluded risk of bias and sensitivity analyses. Following JBI scoping review methodology, quality appraisal of individual studies was not performed or required. The nature of the extracted data precluded quantitative synthesis. The editing of this manuscript was assisted by Claude 3.7 Sonnet, a large language model (LLM) developed by Anthropic.
The LLM was used to identify spelling, grammar, and redundancy errors, and to assist in reducing word count, while the authors made all content decisions, performed analyses, and drew interpretations. This use of AI assistance is disclosed in accordance with the principles of scientific transparency.
Results
Inclusion of sources of evidence
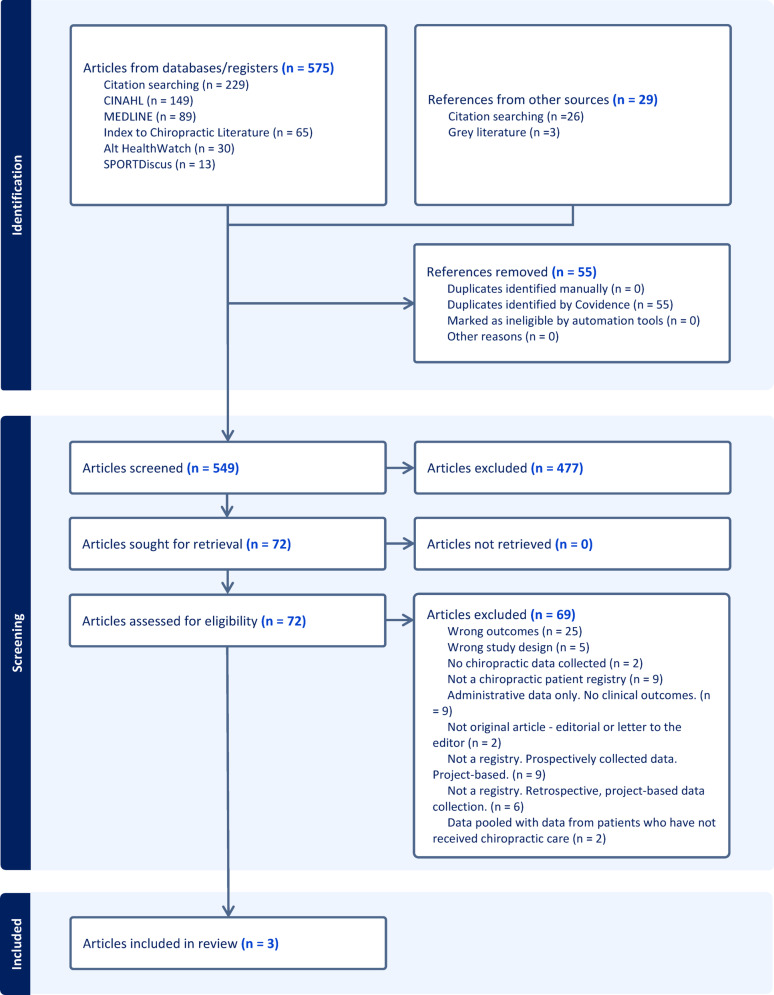
Figure 1 Our search strategy identified 604 evidence sources, with 549 remaining after deduplication in Covidence. Following title and abstract screening with refined definitions and methodology, 477 were excluded. Of the 72 full-text evidence sources assessed for eligibility, three met the inclusion criteria of being a clinical registry that collected chiropractic clinical outcomes data and were selected for data extraction (Figure 1, PRISMA flow diagram). All three evidence sources described Spine IQ. [1, 35, 36]
During our review, we also identified SpineData, a Danish clinical registry of people with low back pain of 2 to 12 months duration. [37, 38] However, after correspondence with the data manager, SpineData did not meet our inclusion criteria as it does not specifically collect outcomes data from chiropractic care, though it does collect spine-related outcomes from a regional non-surgical outpatient clinic.
Although SpineData does not meet the inclusion criteria, we include a discussion of it as it represents a potential opportunity for integration with chiropractic data through its established infrastructure within the Danish healthcare system.
Citation tracking for Spine IQ revealed no publications, explicitly or indirectly, citing registry data.
Characteristics of included studies

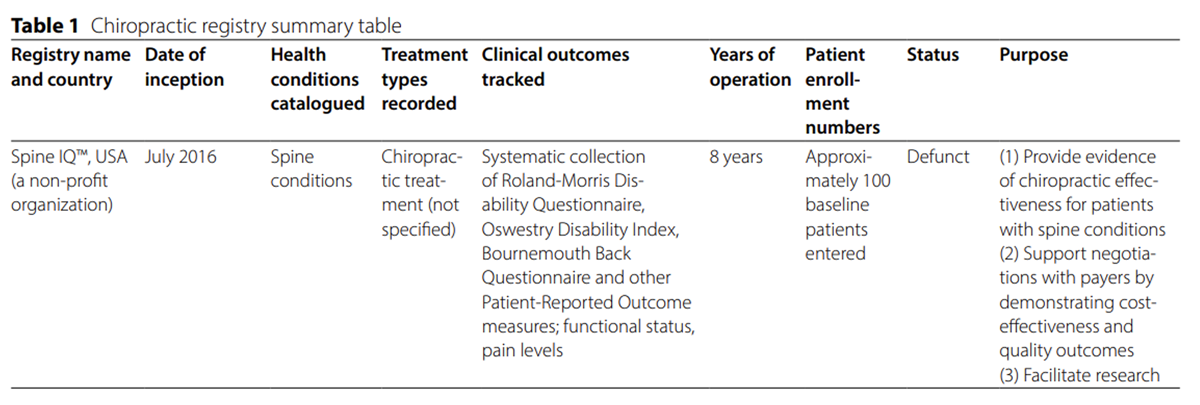
Table 1 The clinical registry characteristics for Spine IQ are shown in Table 1.
Spine IQ
Three abstracts were found in the grey literature that described Spine IQ, published in October 2016, January 2017, and December 2018, respectively. [1, 35, 36] At its launch in July 2016, Spine IQ began with a small cohort of approximately 50 chiropractors submitting data on over 2,000 patients with low back pain. The initial registry focused specifically on outcomes related to back pain from chiropractic treatment. The articles suggest potential future expansion to include data from multiple non-surgical spine care disciplines, such as acupuncture and physical therapy.
Functional outcome measures collected by Spine IQ included the Oswestry Disability Index [39] and Bournemouth Questionnaire [40] for low back pain, and the PROMIS measure of functional status [41] — all with established property measurements and values for minimal clinically important difference (MCID).
The 2017 abstract emphasized using Spine IQ to “harness the power of big data.” The registry gained designation as a Qualified Clinical Data Registry (QCDR) from CMS in 2016, facilitating reimbursements through the Merit-based Incentive Payment System (MIPS) by gathering data via “easy-to-use electronic surveys.” By December 2018, Spine IQ had completed its pilot phase involving 10 chiropractic clinics representing approximately 50 chiropractors nationwide, proving the feasibility of its data collection and reporting systems, with plans to expand to 100 clinics in 2019.
SpineData
Though not meeting our inclusion criteria for a chiropractic clinical outcomes registry, SpineData warrants discussion as a model that could potentially incorporate chiropractic data in the future. SpineData is a clinical outcomes registry tracking patients with low back pain of 2 to 12 months duration the Spine Centre of Southern Denmark, a regional non-surgical outpatient facility at Kolding Hospital. The registry is administered through the University of Southern Denmark with funding from multiple sources, including private organizations (Industriens Arbejdsskadeforsikring and Trygfonden), a project grant from the Danish Foundation for Chiropractic Research and Postgraduate Education, and public funding from the Medical Department of the Spine Centre at Kolding Hospital.
Through personal correspondence with SpineData’s data manager we learned it was established in 2011 and launched operations in 2013, collecting clinical outcomes data on low back, mid-back, and neck pain until June 2021. In 2019 the mid-back and neck regions were combined into a single baseline questionnaire. By the end of May 2021, SpineData had collected 97,521 baseline questionnaires (77,669 complete, 7,104 partially complete, and 12,748 incomplete). SpineData was subsequently replaced by ‘Mine Rygdata’ (MiRD’), described as a ‘re-evaluated version of SpineData with slight modifications in content in structure,’ which collects outcomes data for two bodily regions: (1) low back, and (2) neck or mid-back, with comparable completion rates.
All excluded studies are listed in Appendix 2, Supplementary Materials, with their specific reasons for exclusion.
Discussion
Summary of key findings
This scoping review of chiropractic clinical outcomes registries identified Spine IQ in the U.S. as the profession’s only dedicated registry. The review highlights a significant gap in dedicated chiropractic outcomes registries compared to other healthcare disciplines, particularly orthopedics, which have successfully leveraged registries for research, quality improvement, and evidence-based practice for decades. [2, 42]
The impact of clinical outcomes registries in the chiropractic profession
The establishment of Spine IQ coincided with significant changes to the U.S. healthcare reimbursement landscape, particularly following the passage of the Medicare Access and CHIP Reauthorization Act of 2015. [43]
This legislation established the Merit-Based Incentive Payment System (MIPS) under the Centers for Medicare and Medicaid Services (CMS), which by 2024 had awarded approximately $500 million annually in performance-based bonuses to roughly 572,000 eligible clinicians. Dr. Christine Goertz, DC, PhD, founded Spine IQ with the strategic aim of helping chiropractors demonstrate superior clinical outcomes and potentially secure higher merit-based reimbursements.
The registry accomplished this by implementing serial tracking of up to seven patient-reported outcome measures (PROs) that focused on care effectiveness rather than utilization. Spine IQ’s subsequent designation as a Qualified Clinical Data Registry (QCDR) was crucial as it enabled chiropractors to submit outcomes data directly to CMS’s merit-based incentive system. Despite this infrastructure and potential for financial benefit, chiropractic participation has remained nominal due to limited awareness and adoption within the profession. Currently only one domain — Rehabilitative Support for Musculoskeletal Care — remains open for chiropractic participation. [43]
In contrast to the Spine IQ model in the U.S., SpineData in Denmark [37] represents an alternative approach, though it did not meet our inclusion criteria as a chiropractic-specific registry. Nevertheless, SpineData offers valuable insights as a potential model for future registry development due to its infrastructure and linkage capabilities within the Danish healthcare system.
While it does not currently collect chiropractic clinical outcomes data, SpineData demonstrates the research potential of well-designed clinical outcomes registries. The substantial number of peer-reviewed publications citing SpineData [38, 44–58] illustrates how registry data can generate meaningful research output when adequately established and maintained.
Additionally, SpineData’s evolution into MiRD exemplifies how registries can adapt to changing healthcare needs while preserving data continuity. For the chiropractic profession, SpineData represents a promising opportunity to integrate with established registry frameworks, particularly in countries with nationalized healthcare systems like Denmark where infrastructure for data collection and analysis already exists.
Comparison with other healthcare registries
Since Brand et al. outlined the benefits of clinical registries in 1990 [2], many healthcare professions have successfully leveraged them to advance practice. Technological advances in mobile computing have enabled the automatic delivery of serial PRO questionnaires via email and SMS, allowing for substantial registry development. Modern electronic patient-reported outcomes collection (ePRO) systems have replaced earlier platforms, offering scalable solutions with improved follow-up data collection. [59, 60]
The Multicenter Orthopaedic Outcomes Network (MOON) in the United States exemplifies this success, producing over 40 publications in its first decade. [42] MOON data directly influenced clinical practice by unnecessary interventions, validating specific rehabilitation approaches, and developing standardized rehabilitation protocols. By identifying modifiable outcome predictors that informed meaningful clinical trials, MOON demonstrates how registries can drive evidence-based practice evolution.
Similarly, national joint replacement registries track implant performance and patient outcomes, leading to continuous improvement in surgical techniques and device safety while providing surgeons with performance benchmarking. [61] While other healthcare disciplines have established numerous clinical registries across multiple countries [3, 18, 19, 24, 62–64], chiropractic has lagged in developing this critical research infrastructure.
Comparison with large non-registry databases
Our review also identified non-registry databases that include chiropractic data, such as TriNetX®, a multi-hospital database, and the Danish national health registries. [65, 66] While these databases contain valuable information about chiropractic care utilization and costs, they fundamentally differ from clinical registries in that they lack systematic collection of clinical outcomes data. Furthermore, data from institutional sources like the U.S. Veterans Administration have limited generalizability to independent chiropractic practices — where most patient encounters occur — highlighting gaps that dedicated chiropractic clinical outcomes registries could address. [65]
Barriers to developing chiropractic clinical outcomes registries
Despite the clear benefits of clinical outcomes registries, implementing clinical registries in chiropractic faces numerous interconnected challenges. Financial constraints pose a significant barrier, as registries require substantial investment for infrastructure, data systems, training, and analysis, without the industry partnerships that fund similar efforts in other medical specialties.
Technological challenges compound these issues, as many chiropractic practices lack necessary digital resources, while diverse electronic health records systems impede standardization. Regulatory compliance with privacy frameworks like HIPAA in the U.S. or the General Data Protection Regulation (GDPR) in Europe demands legal expertise beyond many organizations’ capabilities, though standardized de-identification procedures during routine care consent may simplify institutional review requirements.
The profession’s diverse philosophies complicate consensus-building around standardized protocols, while immediate clinical concerns often overshadow long-term data collection priorities. Further challenges include establishing agreement on outcome measures, validated instruments, measurement frequency, and tracked conditions. Without meaningful incentives such as enhanced reimbursements, regulatory mandates, or professional recognition, practitioners remain hesitant to commit necessary resources. Finally, sustainability presents ongoing challenges, as exemplified by the SpineData to MiRD transition, where changes in funding, leadership, technology, and regulations necessitate continuous adaptation and resource commitment.
Future efforts to establish chiropractic clinical outcomes registries will need to address these challenges through collaborative approaches, sustainable funding models, and clear articulation of benefits to all stakeholders.
Stakeholder perspectives on registry development
The development and implementation of chiropractic clinical outcomes registries involves multiple stakeholders, each with distinct perspectives, priorities, and concerns that must be considered for successful implementation. These stakeholders include chiropractors, patients, researchers, healthcare systems, policymakers, and educational institutions. Each group will bring differing perspectives on registries.
Chiropractors may have concerns about workflow disruption and scrutiny while valuing the push toward evidence-based practice. Patients, as stakeholders, balance privacy concerns against strong interest in how their outcomes compare to “patients like me.” Researchers will weigh registry data access challenges against the opportunity to conduct comparative effectiveness studies and garner potential funding for innovative outcomes registry-based projects.
A stakeholder-centered approach that addresses the diverse perspectives and needs of these stakeholders through inclusive planning, clear communication about benefits and expectations, and meaningful engagement throughout the development process will enhance both the initial acceptance and long-term sustainability of chiropractic registries.
Future directions for chiropractic registry development
Based on the findings of this review and the identified gaps, advancing chiropractic clinical registries requires a multifaceted approach including collaborative infrastructure development through partnerships between professional associations, academic institutions, and practice organizations, multi-stakeholder funding models, focused condition-specific registries, and standardized technical specifications. Leveraging technological advances is essential, utilizing mobile and cloud-based technologies, automated follow-up systems, artificial intelligence applications, and user-friendly dashboards that provide real-time feedback.
Strategic alignment with healthcare priorities demands designing registries that address contemporary challenges like non-pharmacological pain management, aligning outcome measures with other disciplines and approaches, enabling comparative clinical and cost-effectiveness analyses, and supporting quality reporting requirements.
Building research capacity involves developing training programs, creating research fellowships, establishing governance structures, and prioritizing publication of findings.
International collaboration requires coordinating across national boundaries to harmonize data elements, learning from existing registries, exploring comparative studies, and developing adaptable resources across care contexts and sub-populations.
Patient engagement necessitates involving patients in registry design, developing explanatory materials, creating feedback mechanisms, and exploring efficient integration of patient-reported outcomes into workflows.
Finally, incentive structures should advocate recognition in reimbursement models and credentialing, develop recognition programs, create clear feedback mechanisms demonstrating contributions to professional advancement, and explore certification programs for practices meeting quality benchmarks.
The development of robust chiropractic clinical outcomes registries represents a significant opportunity for the profession to strengthen its evidence base and credibility, demonstrate value within healthcare systems, and continuously improve quality of care. Strategic investment in this infrastructure would position chiropractic to make meaningful contributions to addressing major global public health challenges related to musculoskeletal pain and function.
Limitations
Our review identified only one chiropractic registry (Spine IQ; U.S.) that met our inclusion criteria. Expanding our criteria to include databases, PBRNs, and other data repositories that capture data related to non-clinical aspects of chiropractic care may also be important to map, although outside the scope of this project.
The review did not conduct a quality assessment of included registries. However, it is worth noting that there are no universally adopted criteria for evaluating clinical outcomes registries, although diverse frameworks exist. [6, 67]
Given the paucity of identified clinical registries, this review lacks comprehensive data on barriers to implementation and adoption specific to chiropractic registries. While we have proposed several barriers based on the literature from other healthcare disciplines [6, 68–70] direct evidence regarding chiropractic-specific challenges is limited.
While we have proposed a framework for considering stakeholder perspectives, this review did not directly capture the views of different stakeholders regarding registry development. Future qualitative research specifically addressing stakeholder perspectives would be valuable for informing implementation strategies.
Conclusions
This scoping review of chiropractic clinical outcomes registries identified Spine IQ in the U.S. as the profession’s only registry. While other registries have the potential for integrating chiropractic data into established healthcare registries, a significant gap remains in dedicated registries within the chiropractic profession. Coordinated efforts among multiple stakeholders are necessary to inform the design and implementation of clinical registries dedicated to chiropractic clinical outcomes.
Supplementary Material
Supplementary Material 1
All search strings used in this study (19.1KB, docx)
Supplementary Material 2
Retrieved publications that were excluded from data extraction (28.1KB, docx)Acknowledgements
The authors would like to acknowledge Kent Murnaghan, MA, MISt of Canadian Memorial Chiropractic College (CMCC) for his performance of the PRESS review of our search strategy, as well as Christine Goertz DC, PhD at Duke University and Natalie Hong Siu Chang at the Spine Centre of Southern Denmark for their helpful correspondence in clarifying registry details.
Author contributions
MM and JC conceived of the study.
AF conducted the evidence search.
JC and KS conducted the data collection
JC and KS extracted and analyzed the data with support from KP and MM.
JC prepared the manuscript with support, contributions, and critical feedback of KS, KP, AF, and MM.
All authors reviewed the manuscript.
Funding
The authors declare they received no funding for this project.
Competing interests
The authors declare no competing interests.
References:
Goertz C.
Clinical data registries deserve your attention.
Dyn Chiropractic. 2017;35(10):60–3.Brand DA, Krag MH, Hausman MR, Trainor KF, Akelman E, et al.
A patient registry for orthopedic surgery.
Clin Orthop Relat Res. 1990;252:262–9Jenio FZ, Scholes C, Marenah M, Li J, Cowley M, et al.
Quality in practice: implementation of a clinical outcomes registry in regenerative medicine.
Ann Transl Med. 2019;7(7):130Khorsan R, Coulter ID, Hawk C, Choate CG.
Measures in chiropractic research: choosing patient-based outcome assessments.
J Manip Physiol Ther. 2008;31(5):355–75.Arts DG, De Keizer NF, Scheffer GJ.
Defining and improving data quality in medical registries: a literature review, case study, and generic framework.
J Am Med Inform Assoc. 2002;9(6):600–11Gliklich RE, Dreyer NA, Leavy MB, Christian JB, eds.
Registries for evaluating patient outcomes: a user’s guide.
4th edition. 4th edition ed. Rockville, MD:
Agency for Healthcare Research and Quality (US); 2020Mold JW, Peterson KA.
Primary care practice-based research networks: working at the interface between research and quality improvement.
Ann Fam Med. 2005;3(Suppl 1):S12-20.Sackett DL, Rosenberg WM, Gray JA, Haynes R.
Evidence-Based Medicine: What It Is and What It Isn't
British Medical Journal 1996 (Jan 13); 312 (7023): 71–72Langley GJ, Nolan KM, Nolan TW, Haynes RB, Richardson WS.
The improvement guide: a practical approach to enhancing organizational performance.
San Francisco: Jossey-Bass; 2009.Nathwani D, Tice A.
Ambulatory antimicrobial use: the value of an outcomes registry.
J Antimicrob Chemother. 2002;49(1):149–54Greenhalgh J, Dalkin S, Gooding K, Gibbons E, et al.
Functionality and feedback: a realist synthesis of the collation, interpretation and utilisation of patient-reported outcome measures data to improve patient care. 2017.
Health Services and Delivery Research. Southampton (UK).Burke LB, Kennedy DL, Miskala PH, Papadopoulos EJ.
The use of patient-reported outcome measures in the evaluation of medical products for regulatory approval.
Clin Pharmacol Ther. 2008;84(2):281–3Gebbie K, Cullen MR.
The Future of Nursing: Leading Change, Advancing Health.
Washington (DC): Institute of Medicine (US),
Nursing CotRWJFIotFo; 2011.Schloss J, McIntyre E, Steel A, Bradley R, et al.
Lessons from outside and within: exploring advancements in methodology for naturopathic medicine clinical research.
J Altern Complem Med. 2019;25(2):135–40.Maruszczyk K, Aiyegbusi OL, Cardoso VR, Gkoutos GV, et al.
Implementation of patient-reported outcome measures in real-world evidence studies: analysis of ClinicalTrials.gov records (1999–2021).
Contemp Clin Trials. 2022;120:106882Huemer M, Bosch F.
Measuring what matters: Why and how to include patient reported outcomes in clinical care and research on inborn errors of metabolism.
J Inherit Metab Dis. 2023;46(5):796–805.Guyatt GH, Sackett DL, Cook DJ.
Users’ guides to the medical literature. II. How to use an article about therapy or prevention. A. Are the results of the study valid?
JAMA. 1993;270(21):2598–601.Cassidy LD, Jensen JN, Durkee CT, Calkins CM, et al.
Creation and implementation of a prospective pediatric clinical outcomes registry.
J Registry Manag. 2011;38(3):138–43.Asher AL, Knightly J, Mummaneni PV, Alvi MA, McGirt MJ, et al.
Quality Outcomes Database Spine Care Project 2012–2020: milestones achieved in a collaborative North American outcomes registry to advance value-based spine care and evolution to the American Spine Registry.
Neurosurg Focus. 2020;48(5):E2.Biant LC, Conley CW, McNicholas MJ.
The first report of the international cartilage regeneration and joint preservation society’s global registry.
Cartilage. 2021;13(1_suppl):74S-81S.Murphy MSQ, Fell DB, Sprague AE, Corsi DJ, Dougan S, Dunn SI, et al.
Data resource profile: better outcomes registry & network (BORN) ontario.
Int J Epidemiol. 2021;50(5):1416–7.Sanderson G, Ariyaratne TV, Wyss J, Looi V.
A global patient outcomes registry: cochlear paediatric implanted recipient observational study (Cochlear(TM) P-IROS).
BMC Ear Nose Throat Disord. 2014;14:10.Edwards ER, Graves SE, McNeil JJ, Williamson OD, Urquhart DM, Cicuttini FM, et al.
Orthopaedic trauma: establishment of an outcomes registry to evaluate and monitor treatment effectiveness.
Injury. 2006;37(2):95–6.Asher AL, Speroff T, Dittus RS, Parker SL, Davies JM, et al.
The national neurosurgery quality and outcomes database (N2QOD): a collaborative North American outcomes registry to advance value-based spine care.
Spine. 2014;39(22 Suppl 1):S106–16.Bliddal M, Broe A, Pottegard A, Olsen J, Langhoff-Roos J.
The Danish medical birth register.
Eur J Epidemiol. 2018;33(1):27–36.Cote P, Negrini S, Donzelli S, Kiekens C, Arienti C, et al.
Introduction to Target Trial Emulation in Rehabilitation:
A Systematic Approach to Emulate a Randomized
Controlled Trial Using Observational Data
Eur J Phys Rehabil Med 2024 (Feb); 60 (1): 145–153Hoffman RL, Bartlett EK, Medbery RL, Sakran JV.
Outcomes registries: an untapped resource for use in surgical education.
J Surg Educ. 2015;72(2):264–70.Thelwall M.
Alternative medicines worth researching? Citation analyses of acupuncture, chiropractic, homeopathy, and osteopathy 1996–2017.
Scientometrics. 2021;126(10):8731–47.Peters M, Godfrey C, McInerney P, Munn Z, Tricco A, Khalil H.
Scoping reviews (2021 version).
JBI Manual for Evidence Synthesis. 2021.Tricco AC, Lillie E, Zarin W, O’Brien KK, Colquhoun H, et al.
PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation.
Ann Intern Med. 2018;169(7):467–73.Peters MDJ, Godfrey C, McInerney P, Khalil H, et al.
Best practice guidance and reporting items for the development of scoping review protocols.
JBI Evid Synth. 2022;20(4):953–68.Carmichael J, Stuber K, Pohlman K, Ferguson A, Maiers M.
Chiropractic clinical registries: A scoping review protocol.
INPLASY protocol 202360064. 2023. 10.37766/inplasy2023.6.0064McGowan J, Sampson M, Salzwedel DM, Cogo E, Foerster V, Lefebvre C.
PRESS peer review of electronic search strategies: 2015 guideline statement.
J Clin Epidemiol. 2016;75:40–6.Haddaway NR, Grainger MJ, Gray CT.
citationchaser: An R package and Shiny app for forward and backward citations chasing in academic searching.
Zenodo [Internet]. 2021 February 21-23, 2025.
Available from: https://zenodo.org/records/4543513Goertz C.
Transitioning from volume to value in the chiropractic office.
Am Chiropract. 2017;39(1):34–5.Goertz C.
Using data to explain chiropractic outcomes: interview with Christine Goertz, DC, PhD.
Am Chiropract; 2018. p. 34–40.Kent P, Kongsted A, Jensen TS, Albert HB, Schiottz-Christensen B.
SpineData—a Danish clinical registry of people with chronic back pain.
Clin Epidemiol. 2015;7:369–80.Ranger TA, Cicuttini FM, Jensen TS, Heritier S, Urquhart DM.
Paraspinal muscle cross-sectional area predicts low back disability but not pain intensity.
Spine J. 2018;19(5):862–8.Copay AG, Glassman SD, Subach BR, Berven S, Schuler TC.
Minimum clinically important difference in lumbar spine surgery patients: a choice of methods using the Oswestry Disability Index, Medical Outcomes Study questionnaire Short Form 36, and pain scales.
Spine J. 2008;8(6):968–74.Newell D, Bolton JE.
Responsiveness of the Bournemouth questionnaire in determining minimal clinically important change in subgroups of low back pain patients.
Spine. 2010;35(19):1801–6.Sandal LF, Young JJ, Sogaard K, Hartvigsen J.
Convergent and discriminative validity of the PROMIS physical function 4 questionnaire for assessing pain-related disability in low back pain patients seeking chiropractic care.
Spine. 2022;47(18):1314–20.Lynch TS, Parker RD, Patel RM, Andrish JT, Group M, et al.
The impact of the multicenter orthopaedic outcomes network (MOON) research on anterior cruciate ligament reconstruction and orthopaedic practice.
J Am Acad Orthop Surg. 2015;23(3):154–63.(CMS) USCfMMS.
Explore MIPS Value Pathways (MVPs) Baltimore, MD:
U.S. Centers for Medicare & Medicaid Services; 2024
[This website indicates that there is only one current registry open to application from chiropractors, “Rehabilitative Support for Musculoskeletal Care,” which seeks to promote quality rehabilitative care for patients. The reporting of outcome measures for back or neck impairments are required as one of four quality measures to qualify for this merit-based incentive payment system (MIPS).].
Available from: https://qpp.cms.gov/mips/
explore-mips-value-pathways/2024/M1370O’Neill S, Jensen TS, Kent P.
Computerized quantification of pain drawings.
Scand J Pain. 2019;20(1):175–89.Ipsen JA, Sandal LF, Chang NHS, Schiřttz-Christensen B.
Interest in mHealth among patients with low back pain: cross-sectional study.
JMIR Hum Factors. 2024;11:e48729.Manniche C, Stokholm L, Ravn SL, Andersen TE, et al.
Long-term opioid therapy in spine center outpatients: protocol for the spinal pain opioid cohort (SPOC) study.
JMIR Res Protoc. 2020;9(8):e21380.Chang NHS, Nim C, Harsted S, Young JJ, O’Neill S.
Data-driven identification of distinct pain drawing patterns and their association with clinical and psychological factors: a study of 21,123 patients with spinal pain.
Pain. 2024;165(10):2291–304Harsted S, Chang NHS, Nim C, Young JJ, McNaughton DT, O’Neill S.
Exploring the association between patient-drawn pain diagrams and psychological and physical health variables: a large-scale study of patients with low back pain.
Eur J Pain (London, England). 2024;29(2):e4711.Clausen S, Hartvigsen J, Johansson MS, Kjřnř LG, et al.
Healthcare utilisation in danish primary care among patients with low back or neck/thoracic spine pain before and after assessment in secondary care.
Musculoskeletal Care. 2024;22(4):1–9.Mihlberg E, Arnbak BA-M.
Prognostic factors for long-term improvement in pain and disability among patients with persistent low back pain.
Chiropr Man Ther. 2024;32(1):26Arnbak B, Jensen TS, Hendricks O, Řstergaard M, et al.
Prognostic value of the clinical and imaging arm of the ASAS criteria for progression of structural sacroiliac joint lesions.
Mod Rheumatol. 2022;34(2):391–8.Arnbak B, Jensen RK, Manniche C, Hendricks O, et al.
Identification of subgroups of inflammatory and degenerative MRI findings in the spine and sacroiliac joints: a latent class analysis of 1037 patients with persistent low back pain.
Arthritis Res Ther. 2016;18(1):237.Arnbak B, Jensen TS, Schiřttz-Christensen B, et al.
What level of inflammation leads to structural damage in the sacroiliac joints? A four-year magnetic resonance imaging follow-up study of low back pain patients.
Arthritis Rheumatol (Hoboken, NJ). 2019;71(12):2027–33Arnbak B, Jurik AG, Hřrslev-Petersen K, Hendricks O, et al.
Associations between spondyloarthritis features and magnetic resonance imaging findings: a cross-sectional analysis of 1,020 patients with persistent low back pain.
Arthritis Rheumatol (Hoboken, NJ). 2016;68(4):892–900Arnbak B, Jurik AG, Jensen RK, Schiřttz-Christensen B.
The diagnostic value of three sacroiliac joint pain provocation tests for sacroiliitis identified by magnetic resonance imaging.
Scand Journal Rheumatol. 2016;46(2):130–7.Arnbak B, Jurik AG, Jensen TS, Manniche C.
Association between inflammatory back pain characteristics and magnetic resonance imaging findings in the spine and sacroiliac joints.
Arthritis Care Res (Hoboken). 2018;70(2):244–51.Jensen RK, Dissing KB, Jensen TS, Clausen SH, Arnbak B.
The Association Between Cervical Degenerative MRI Findings
and Self-reported Neck Pain, Disability and Headache:
A Cross-sectional Exploratory Study
Chiropractic & Manual Therapies 2023 (Oct 11); 31: 45Kiil RM, Arnbak B, Zejden A, Schiřttz-Christensen B.
Pregnancy-related sacroiliac joint findings in females with low back pain: a four-year magnetic resonance imaging follow-up study.
Acta Radiol. 2021;63(6):2841851211017108.Fidai MS, Saltzman BM, Meta F, Lizzio VA, Stephens JP, Bozic KJ, et al.
Patient-reported outcomes measurement information system and legacy patient-reported outcome measures in the field of orthopaedics: a systematic review.
Arthroscopy. 2018;34(2):605–14.Wicks P, Hotopf M, Narayan VA, Basch E, Weatherall J, Gray M.
It’s a long shot, but it just might work! Perspectives on the future of medicine.
BMC Med. 2016;14(1):176.Heckmann N, Ihn H, Stefl M, Etkin CD, Springer BD, Berry DJ, et al.
Early results from the american joint replacement registry: a comparison with other national registries.
J Arthroplast. 2019;34(7S):S125-S34e1.Gressler LE, Devlin V, Jung M, Marinac-Dabic D, et al.
Orthopedic coordinated registry network (Ortho-CRN): advanced infrastructure for real-world evidence generation.
BMJ Surg Interv Health Technol. 2022;4(Suppl 1): e000073.Capo-Lugo CE, Kho AN, O’Dwyer LC, Rosenman MB.
Data sharing and data registries in physical medicine and rehabilitation.
PM R. 2017;9(5S):S59–74.Wasserstein D, Sheth U.
Administrative databases in sports medicine research.
Clin Sports Med. 2018;37(3):483–94.Trager RJ, Daniels CJ, Perez JA, Casselberry RM, Dusek JA.
Association between chiropractic spinal manipulation and lumbar discectomy in adults with lumbar disc herniation and radiculopathy: retrospective cohort study using United States’ data.
BMJ Open. 2022;12(12):e068262.Hartvigsen J, Davidsen M, Sogaard K, Roos EM, Hestbaek L.
Self-reported musculoskeletal pain predicts long-term increase in general health care use: a population-based cohort study with 20-year follow-up.
Scand J Public Health. 2014;42(7):698–704.iNiTiative PTPR.
Methodological guidelines and recommendations for efficient and rational governance of patient registries.
Slovenia: National Institute of Public Health Slovenia; 2015.Gliklich RE, Leavy MB, Karl J, Campion DM, Levy D, Berliner E.
A framework for creating standardized outcome measures for patient registries.
J Comp Eff Res. 2014;3(5):473–80.Hoque DME, Kumari V, Hoque M, Ruseckaite R, Romero L.
Impact of clinical registries on quality of patient care and clinical outcomes: a systematic review.
PLoS ONE. 2017;12(9):e0183667.Stey AM, Russell MM, Ko CY, Sacks GD, Dawes AJ, Gibbons MM.
Clinical registries and quality measurement in surgery: a systematic review.
Surgery. 2015;157(2):381–95.
Return to ALL ABOUT CHIROPRACTIC
Since 6-21-2026
| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |