

Prevalence of Low Back Pain in Adolescents with
Idiopathic Scoliosis: A Systematic ReviewThis section was compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: Chiropractic & Manual Therapies 2017 (Apr 20); 25: 10 ~ FULL TEXT
OPEN ACCESS Jean Théroux, Norman Stomski, Christopher J. Hodgetts, Ariane Ballard,
Christelle Khadra, Sylvie Le May and Hubert Labelle
Research Center,
Sainte-Justine University Hospital Center
School of Health Profession,
Murdoch UniversityBackground Adolescent idiopathic scoliosis is the most common spinal deformity occurring in adolescents and its established prevalence varies from 2 to 3%. Adolescent idiopathic scoliosis has been identified as a potential risk factor for the development of low back pain in adolescents. The purpose of this study was to systematically review studies of the prevalence of low back pain in adolescents with idiopathic scoliosis in order to establish the quality of the evidence and determine whether the prevalence estimates could be statistically pooled.
Methods Systematic electronic searches were undertaken in PubMed, CINAHL, and CENTRAL without any restrictions. Studies were eligible for inclusion if they reported the prevalence of low back pain in adolescents with idiopathic scoliosis. Studies were excluded if they detailed the prevalence of pain in post-surgical subjects or were published in languages other than English or French. Data were reported qualitatively, since there was insufficient evidence for statistical pooling.
Results The electronic search strategies yielded 1811 unique studies. Only two studies fulfilled the eligibility criteria. The prevalence of low back pain in adolescents with idiopathic scoliosis ranged from 34.7 to 42.0%. However, these prevalence estimates should be viewed cautiously as the included studies were at high risk of bias.
Conclusion The results of this systematic review indicate that adolescents with idiopathic scoliosis frequently experience low back pain. However, there was insufficient evidence to confidently estimate low back pain prevalence in adolescents with idiopathic scoliosis and further studies are needed in this area.
Keywords Low back pain Adolescent idiopathic scoliosis Prevalence
From the Full-Text Article:
Introduction
In developed countries, low back pain commonly occurs and is a leading cause of disability and financial burden. [1] The epidemiology of low back pain has been extensively researched in adults but is less well understood in adolescents. [2] Estimates of the prevalence of low back pain in adolescents vary widely, but a recent systematic review concluded that the 1–week prevalence was 17.7%, and 12–month prevalence was 33.6%. [3] Low back pain impacts significantly on adolescents, as over nine in ten report disability that may include reduced physical activity, school absenteeism, and limitations in daily activities. [4–6]
The Scoliosis Research Society defines adolescent idiopathic scoliosis as a three-dimensional spinal deviation with a greater than 10° Cobb angle of unknown aetiology occurring in adolescents 10 years and older. [7] Adolescent idiopathic scoliosis is the most common spinal deformity occurring in adolescents and its established prevalence varies from 2 to 3%. [8] Adolescent idiopathic scoliosis has been identified as a potential risk factor for the development of low back pain in adolescents. [9] Subsequently, studies have been undertaken to establish the prevalence of low back pain in adolescents with idiopathic scoliosis.
Literature reviews have detailed the prevalence of back pain, but not specifically low back pain, in adolescents with idiopathic scoliosis. [10] Moreover, such reviews have not assessed the quality of the available evidence, and therefore have not established whether estimates of back pain prevalence may be subject to bias. [10] Hence, the purpose of this study was to systematically review studies examining the prevalence of low back pain in adolescents with idiopathic scoliosis in order to establish the quality of the evidence and determine whether the prevalence estimates could be statistically pooled.
Methods
The methods used in this review accorded with PRISMA recommendations and the Methodological Evaluation of Observational Research guidelines. [11, 12]
Search strategy
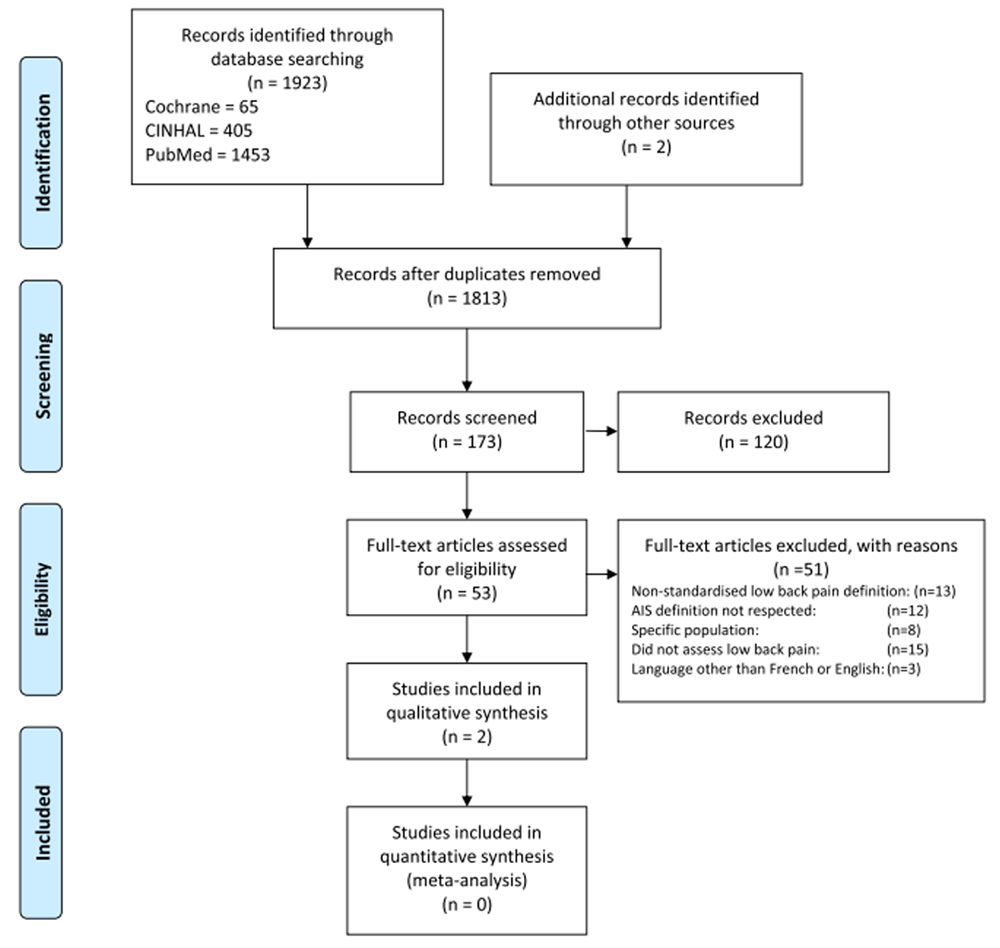
Figure 1 Figure 1 displays the search strategies implementation and selection of studies. Database specific search strategies were developed to retrieve English or French language studies that detailed the prevalence of low back pain in adolescent idiopathic scoliosis populations. PubMed, CINAHL, and CENTRAL were searched without any restrictions.
Additional file 1 presents the PubMed, CINAHL, and CENTRAL search strategies. The titles and abstracts of the studies retrieved through the searches were independently screened by two reviewers to identify potentially relevant studies that reported the prevalence of low back pain in adolescents with idiopathic scoliosis. In addition, citations in these identified studies were inspected to identify additional relevant studies. Two reviewers obtained full-text copies of all potentially relevant studies and considered them for inclusion in this review.
Selection criteria
Any study that reported the prevalence of low back pain in adolescents with idiopathic scoliosis was considered for inclusion in this study. Adolescent idiopathic scoliosis was defined as a spinal deviation greater than 10° in adolescents aged between 10 and 17 years old. [7] Low back pain was defined as pain located on the posterior aspect of the body from the lower margin of the 12th rib to the lower gluteal folds. [13] Studies were excluded if they detailed the prevalence of pain in post-surgical subjects or were published in languages other than English or French.
Data extraction
One reviewer extracted data from the included studies into an Excel database. Only raw, aggregated prevalence data were extracted since the reported data in the included studies were not standardised or stratified by age, gender or other demographic characteristics. Low back pain case definitions were segmented according to minimum duration of low back pain episode and anatomic location of pain. Other extracted data included: study type, publication date, country, sample size, age, gender, prevalence period, Cobb angle, and data used to assess risk of bias.
Assessment of risk of bias for included studies
Two reviewers assessed risk of bias for each included study, using a reliable purpose built tool. [14] This tool comprises 10 items that evaluate measurement bias, selection bias, and bias resulting from the analysis method. Discrepancies in the risk of bias assessment were resolved through consensus.
Data analysis
All data were extracted into spreadsheets and then compared between reviewers to ensure consistency. Prevalence estimates were reported qualitatively since there was insufficient data for statistical pooling.
Grading the strength of evidence
The GRADE Working Group grades of evidence were used to establish the overall strength of the evidence. [15] These grades are as follows:
High quality: Further research very unlikely to alter confidence in the estimate of effect.
Moderate quality: Further research likely to have an important impact on confidence in the estimate of effect and may change the estimate.
Low quality: Further research very likely to have an important impact on confidence in the estimate of effect and is likely to change the estimate.
Very low quality: Any estimate is very uncertain.
Results
Study selection
The electronic search strategies yielded 1811 unique studies (Fig. 1). Abstract and title screening identified 51 potentially relevant studies, for which full-text articles were retrieved and assessed for eligibility. An additional two potentially relevant studies were identified through inspection of the reference lists in the retrieved full-text articles. Of the retrieved full-text articles, two satisfied the eligibility criteria and were included in this review. [16, 17]
Study characteristics

Table 1 Table 1 displays the included studies’ characteristics. All included studies used cross-sectional study designs and assessed low back pain through self-report questionnaires. In one study 85% of the respondents were female [16] and in the other study, all respondents were female.[17] The mean age of the respondents in one study was 14.2 years [16], and 14.7 years in the other study.[17] One study was conducted in Canada [16] and the other study was undertaken in Japan.[17] Neither of the prevalence estimates was standardised by age, gender, or other demographic characteristics.
Definitions of adolescent idiopathic scoliosis
Both included studies defined the eligibility criteria for adolescent idiopathic scoliosis as people aged 10–17 years with a Cobb angle of more than 10°.[16, 17]
Prevalence of low back pain and prevalence period
In one study the prevalence of low back pain was 42.0% with a prevalence period of the prior 24 h [16], and in the other study low back pain prevalence was 34.7% with a prevalence period of 1 week. [17] Neither of the included studies reported confidence intervals or other forms of error margins.
Case definitions
Neither study reported minimum episode duration required to establish a case of low back pain. The anatomic location of pain was detailed as “low back pain” in one study [17] and “‘lumbar” in the other study [16], but neither study precisely specified the regions encompassed by these locations.
Risk of bias
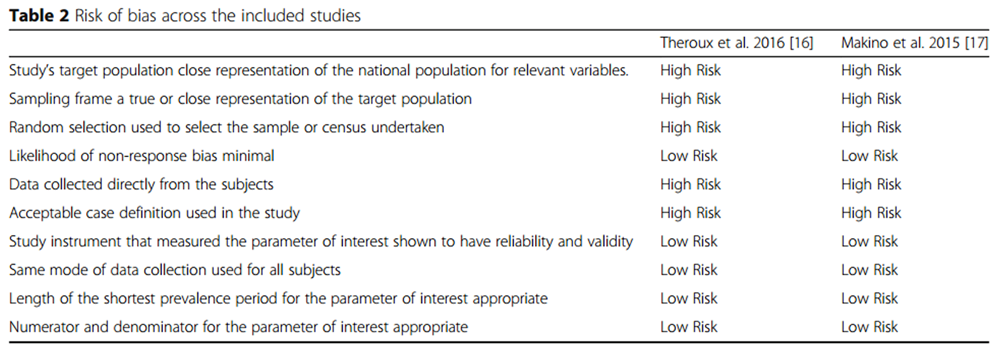
Table 2 Table 2 summarises the risk of bias assessment. Both studies were at high risk of bias for five items.
Overall strength of the evidence
The overall strength of the evidence was considered to be very low quality, in terms of GRADE classifications.
Discussion
This systematic review was the first to assess the prevalence of low back in adolescent idiopathic scoliosis. The findings show that the prevalence of low back pain in adolescents with idiopathic scoliosis ranges from 34.7 to 42.0%. However, the results of this review are based on a limited number of studies at substantial risk of bias. Subsequently, further studies are very likely to have a significant impact on estimates of low back pain prevalence in adolescents with idiopathic scoliosis.
Taken at face value, our findings suggest that over one-third of adolescents with idiopathic scoliosis experience low back pain. In contrast, a recent systematic review of low back pain in the general adolescent population found that the point prevalence was 12.0% and 1–week prevalence was 17.7%. [3] This tentatively suggests that adolescents with idiopathic scoliosis may be at least twice as likely to experience low back pain as adolescents without scoliosis. Again though, additional studies are required to improve the precision of estimates of low back pain in adolescents with idiopathic scoliosis.
The results of this systematic review have identified numerous methodological limitations in prevalence studies of pain in adolescents with idiopathic scoliosis. One such limitation involved the use of unclear definitions of low back pain. Some of the excluded studies reported the prevalence of back pain, but could not be included since it was unclear if the pain was located in the low back or other regions of the back. Hence, the location of back pain should be reported according to standardised anatomic definitions in subsequent studies. [13]
Another limitation of low back pain prevalence studies in adolescent idiopathic scoliosis was the lack of longitudinal monitoring. Without such longitudinal studies, it cannot be established whether cases of low back pain are acute, brief and transitory, or if these cases are recurrent or chronic. [18, 19] It is important to establish whether cases of low back pain in adolescent scoliosis are chronic or recurrent since in these instances the impact on quality of life and burden are likely to be worse than in acute cases. [20, 21] Hence, longitudinal studies of low back pain in adolescent idiopathic scoliosis are warranted, and the findings should be reported by using standardised definitions of low back pain episodes. [22, 23]
Notably omitted from the included studies was the presentation of confidence intervals or other forms of error margins. The lack of error margins makes it difficult to discern the precision of the low back pain prevalence estimates. [24] Also, the omission of error margins does not enable statistical pooling. Error margins can generally be estimated from other data presented in articles or data derived from other sources, but the interpretation of the prevalence estimates detailed in articles would be much enhanced by the presentation of error margins. [24]
The lack of demographic factor segmentation was also a methodological shortcoming of the included studies. While one of the included studies had a gender distribution that was close to typical of the occurrence of idiopathic scoliosis in adolescents, the other study’s sample consisted completely of females. Such imbalances may bias the estimation of low back pain prevalence. [25] Also, none of the studies reported pain prevalence by age bands. If data were broken down by age segments, then it would be possible to establish the trajectory of low back pain prevalence in adolescent idiopathic scoliosis. Finally, low back pain prevalence in adolescent scoliosis should also be classified according to socio-economic status, as it has been associated low back pain in general adolescent populations. [25, 26]
The final main limitation of the included studies that needs to be considered was the selection of study samples. In the included studies, the sample sizes were relatively modest and drawn from a single location. Such samples may lead to selection bias, and population-based studies are required to address this issue. [25]
Limitations
The findings of this review are likely to be influenced by publication bias that may have inflated the estimates of low back pain prevalence in adolescents with idiopathic scoliosis. [27] However, an extensive search was undertaken to identify potentially relevant studies, which should mitigate the impact of publication bias. Also, the risk of bias was assessed for each included prevalence estimate, and we have drawn careful, tentative conclusions on the basis of this assessment.
Conclusion
The results of this systematic review indicate that adolescents with idiopathic scoliosis frequently experience low back pain. However, there was insufficient evidence to confidently estimate low back pain prevalence in adolescents with idiopathic scoliosis and further studies are needed in this area. Moreover, the studies included in this review had numerous methodological weaknesses that researchers should address in subsequent studies. Such limitations include the use of standardised definitions of anatomic low back pain location and episode durations; reporting of prevalence error margins; segmentation of low back pain prevalence by relevant demographic characteristics; monitoring of low back pain prevalence at regular intervals over extended periods; and the use of population-based study cohorts.
Additional file 1:
Appendix 1. Search strategy. (DOC 96 kb)
Authors’ contributions
Conception and design: JT, NS, CH, SL, CK, AB, HL. Analysis: JT, CH, NS. Drafting of the article: NS, JT, CH, SL, CK, AB. Critical revision of the article: NS, JT, CH, SL, CK, AB, HL. Final approval of the article: NS, JT, CH, SL, CK, AB, HL. All authors read and approved the final manuscript.
Competing interests
Norman Stomski is secretary to the editorial team of the journal Chiropractic & Manual Therapies. The other authors declare that they have no competing interests.
Funding
The manuscript submitted does not contain information about medical device(s) / drug(s). No funds were received in support of this work.
References:
Vos T, Flaxman AD, Naghavi M, Lozano R, Michaud C, et al.:
Years Lived with Disability (YLDs) for 1160 Sequelae of 289 Diseases and Injuries 1990-2010:
A Systematic Analysis for the Global Burden of Disease Study 2010
Lancet. 2012 (Dec 15); 380 (9859): 2163–2196Jeffries LJ, Milanese SF, Grimmer-Somers KA.
Epidemiology of Adolescent Spinal Pain:
A Systematic Overview of the Research Literature
Spine (Phila Pa 1976). 2007 (Nov 1); 32 (23): 2630–2637Calvo-Munoz I, Gomez-Conesa A, Sanchez-Meca J.
Prevalence of Low Back Pain in Children and Adolescents:
A Meta-analysis
BMC Pediatr. 2013 (Jan 26); 13: 14Watson KD, Papageorgiou AC, Jones GT, Taylor S, Symmons DP, Silman AJ.
Low back pain in schoolchildren: occurrence and characteristics.
Pain. 2002;97(1–2):87–92.Skoffer B.
Low back pain in 15- to 16-year-old children in relation to school furniture
and carrying of the school bag.
Spine. 2007;32(24):E713–7.Bejia I, Abid N, Ben Salem K, Letaief M, Younes M, Touzi M, Bergaoui N.
Low back pain in a cohort of 622 Tunisian schoolchildren and adolescents:
an epidemiological study.
Eur Spine J. 2005;14(4):331–6.Negrini S, Hresko TM, O’Brien JP, Price N.
Recommendations for research studies on treatment of idiopathic scoliosis:
Consensus 2014 between SOSORT and SRS non-operative management committee.
Scoliosis. 2015;10:8.Wong HK, Tan KJ.
The natural history of adolescent idiopathic scoliosis.
Indian J Orthop. 2010;44(1):9–13.Kovacs FM, Gestoso M, Gil Del Real MT, Lopez J, Mufraggi N, Mendez JI.
Risk factors for non-specific low back pain in schoolchildren and their parents:
a population based study.
Pain. 2003;103(3):259–68.Balague F, Pellise F.
Adolescent idiopathic scoliosis and back pain.
Scoliosis Spinal Disord. 2016;11(1):27.Shamliyan T, Ansari MT, Raman G, Berkman N, Grant M, Janes G.
Development and Implementation of the Standards for Evaluating and Reporting
Epidemiologic Studies on Chronic Disease Incidence or Prevalence.
Am J Public Health Res. 2013;1(7):183–90.Moher D, Liberati A, Tetzlaff J, Altman DG.
Preferred Reporting Items for Systematic Reviews
and Meta-Analyses: The PRISMA Statement
PLoS Medicine 2009 (Jul 21); 6 (7): e1000100Dionne CE, Dunn KM, Croft PR, Nachemson AL, Buchbinder R, Walker BF, et al.
A consensus approach toward the standardization of back pain definitions
for use in prevalence studies.
Spine. 2008;33(1):95–103.Hoy D, Brooks P, Woolf A, Blyth F, March L, Bain C, Baker P, Smith E.
Assessing risk of bias in prevalence studies: modification of an existing tool
and evidence of interrater agreement.
J Clin Epidemiol. 2012;65(9):934–9.Oxman AD, Group GW.
Grading quality of evidence and strength of recommendations.
BMJ. 2004;328(19):1490–4.Theroux J, Le May S, Hebert JJ, Labelle H.
Back Pain Prevalence is Associated with Curve-type and Severity in Adolescents
with Idiopathic Scoliosis: a cross-sectional Study.
Spine. 2016. Epub ahead of print. doi:10.1097/BRS.0000000000001986.Makino T, Kaito T, Kashii M, Iwasaki M, Yoshikawa H.
Low back pain and patient-reported QOL outcomes in patients with adolescent
idiopathic scoliosis without corrective surgery.
Springerplus. 2015;4:397.Kongsted A, Kent P, Axen I, Downie AS, Dunn KM.
What Have We Learned From Ten Years of Trajectory Research in Low Back Pain?
BMC Musculoskelet Disord. 2016 (May 21); 17 (1): 220Axen I, Leboeuf-Yde C.
Trajectories of Low Back Pain
Best Pract Res Clin Rheumatol. 2013 (Oct); 27 (5): 601–612Da C Menezes Costa L, Maher CG, Hancock MJ, McAuley JH, Herbert RD, Costa LO.
The prognosis of acute and persistent low-back pain: a meta-analysis.
CMAJ. 2012;184(11):E613–24.Heuch I, Foss IS.
Acute low back usually resolves quickly but persistent low back pain often persists.
J Physiother. 2013;59(2):127.Stanton TR, Latimer J, Maher CG, Hancock MJ.
How do we define the condition ‘recurrent low back pain’? a systematic review.
Eur Spine J. 2010;19(4):533–9.de Vet HC, Heymans MW, Dunn KM, Pope DP, van der Beek AJ, Macfarlane GJ.
Episodes of low back pain: a proposal for uniform definitions
to be used in research.
Spine. 2002;27(21):2409–16.Vandenbroucke JP, von Elm E, Altman DG, Gotzsche PC, Mulrow CD, Pocock SJ.
Strengthening the Reporting of Observational Studies in Epidemiology (STROBE):
explanation and elaboration.
Plos Med. 2007;4(10):e297.Hoy D, Brooks P, Blyth F, Buchbinder R.
The epidemiology of low back pain.
Best Pract Res Clin Rheumatol. 2010;24(6):769–81.Hestbaek L, Korsholm L, Leboeuf-Yde C, Kyvik KO.
Does socioeconomic status in adolescence predict low back pain in adulthood?
a repeated cross-sectional study of 4,771 Danish adolescents.
Eur Spine J. 2008;17(12):1727–34.Alderson P, Green S.
Cochrane Collaboration open learning material for reviewers, version 1.1.
Cochrane Collaboration; 2002.
Return to SCOLIOSIS
Since 4-22-2017

| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |