

Management of Chronic Low Back
Pain in Active IndividualsThis section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: Curr Sports Med Rep 2010 (Jan); 9 (1): 60–66 ~ FULL TEXT
OPEN ACCESS Mayer JM, Haldeman S, Tricco AC, Dagenais S.
College of Medicine and School
of Physical Therapy and Rehabilitation Sciences,
University of South Florida, Tampa, FL 33612, USA.
jmayer2@health.usf.edu
Chronic low back pain (LBP) is a common and potentially disabling condition in all adults, including those who are physically active. It currently is challenging for clinicians and patients to choose among the numerous treatment options. This review summarizes recommendations from recent clinical practice guidelines and systematic reviews about common primary care and secondary care approaches to the management of chronic LBP. The best available evidence currently suggests that in the absence of serious spinal pathology, nonspinal causes, or progressive or severe neurologic deficits, the management of chronic LBP should focus on patient education, self-care, common analgesics, and back exercises. Short-term pain relief may be obtained from spinal manipulative therapy or acupuncture. For patients with psychological comorbidities, adjunctive analgesics, behavioral therapy, or multidisciplinary rehabilitation also may be appropriate. Given the importance of active participation in recovery, patient preference should be sought to help select from among the recommended treatment options.
From the FULL TEXT Article:
INTRODUCTION
Despite continued research efforts and the development of innovative new interventions in recent decades, low back pain (LBP) remains a prevalent, disabling, costly, and clinically challenging disorder for adults in the United States. The lifetime prevalence of LBP in the general adult population is estimated at 85%, with a 1-yr prevalence of 75% and a point prevalence of 35%. [11] Data from the Medical Expenditure Panel Survey (MEPS) suggest that the annual direct costs of treatment for LBP and neck pain in the United States have increased by 65% from 1997 to 2005, when they reached $86 billion. [34] Despite these rising costs, the proportion of adults who reported functional limitations from LBP or neck pain increased by 19% during the same period. [34]
Unlike many other disorders that primarily affect specific segments of the population, everyone is at risk for LBP regardless of age, sex, occupation, income, education, or location. [33] LBP is prevalent in physically active adults, which is defined as those engaging in the minimum amount of physical activity required to maintain health and reduce the risk for chronic disease. To achieve this physical activity level, the American College of Sports Medicine and the American Heart Association recommend engaging in cardiovascular exercise that is of moderate intensity 5 d·wk–1 for 30 min·d–1 or vigorous intensity 3 d·wk–1 for 20 min·d–1, and resistance training with 8-12 repetitions of 8-10 exercises for 2 d·wk–1. [24] It has been reported that approximately 36% of U.S. adults regularly achieve the levels required to be considered physically active. [5]
Increased risks for LBP and structural abnormalities in the lumbar spine have been reported in various categories of athletes, including gymnasts, American football linesmen, wrestlers, divers, and power lifters. [9, 28, 38, 47] However, the precise relationship between physical activity and LBP is currently unclear. Some studies have suggested that either too little or too much physical activity may increase the risk of LBP [27], while others have found that neither physical activity alone nor a sedentary lifestyle alone is an independent risk factor for LBP. [13, 30] Regardless of the precise relationship between physical activity and LBP, there is no evidence to suggest that the management of LBP should be different in physically active adults than that recommended for the general population.
The assessment of LBP can be simplified through sequential triage by first eliminating rare instances of serious spinal pathology (e.g., fracture, infection, malignancy, cauda equina syndrome, systemic inflammatory disease), nonspinal causes (e.g., genitourinary or gastrointestinal disorders), and severe or progressive neurologic deficits.
The remaining large majority (>95%) of patients without these rare causes of LBP can be deemed to have nonspecific, common LBP for which it is not possible to establish a specific anatomical diagnosis. LBP can then be categorized as acute (<6 wk), subacute (6-12 wk), or chronic (>12 wk) according to duration of symptoms to help inform management. The latter two categories often are combined because recommendations for management are similar. [41]
Episodes of acute LBP usually have a favorable prognosis, with symptoms typically improving within a few weeks and resolving within a few months, with or without treatment. [40] Episodes of LBP that persist beyond 6 wk are less likely to resolve spontaneously and face a poorer prognosis without appropriate management. The progression from acute to chronic LBP likely involves a complex interaction of physical, psychological, socioeconomic, and occupational factors. [50] The management of chronic LBP and its associated disability remains troublesome for patients, clinicians, third-party payers, and policy makers, as a minority of patients with prolonged symptoms account for a majority of costs. [18]
Considering that the etiology of most chronic LBP is unclear, it is not surprising that hundreds of treatment options are now available, including various types of medications, manual therapies, exercise therapies, physical modalities, educational therapies, behavioral therapies, complementary and alternative medicine (CAM) therapies, injection therapies, minimally invasive therapies (e.g., injections), and surgical therapies. This array of treatment options has proliferated largely in the absence of solid evidence to support their efficacy, safety, and cost-effectiveness. The current approach to selecting a particular therapy for chronic LBP in the absence of compelling evidence has been compared to shopping in a supermarket, where large inventories of treatment options are available in each aisle, competing for market share by advertising directed at clinicians and patients, who are both hungry for answers to this vexing problem. [22]
The difficulty with the supermarket approach to chronic LBP is that none of the parties involved appear satisfied. Patients living with chronic LBP must try to choose from among treatment options based on insufficient or even misleading information and face the possibly long-term consequences of their decisions, such as experiencing treatment-related harms, high costs, and poor long-term outcomes. Clinicians routinely are called upon to recommend treatments for chronic LBP without clear direction from the literature or sufficient training in this area. Third-party payers and policy makers often are overwhelmed or frustrated by the general lack of clinical improvement in patients with chronic LBP despite rising costs and must make decisions about reimbursement without clear evidence of cost-effectiveness. [22] Although evidence-based medicine offers an alternative to this supermarket approach, the generally poor long-term outcomes observed with any intervention for chronic LBP often have obscured attempts to reconcile conflicting or limited evidence with the demands of clinical practice.
The objective of this study was to summarize recommendations from recent, evidence-based clinical practice guidelines (CPGs) related to the management of chronic LBP, as well as systematic or narrative reviews on various specific interventions that were published in a special focus issue of The Spine Journal devoted to "evidence informed management of chronic low back pain without surgery." The summary is intended to provide guidance to clinicians on the recommended management of nonspecific, chronic LBP in physically active adults.
METHODS
To identify recently published CPGs, electronic searches were conducted in Medline by combining terms commonly used for guidelines and LBP (e.g., [guideline OR practice guideline] AND low back pain) using the OVID Interface for the period 2005 to October Week 2 2009. Unpublished CPGs were identified by searching the National Guidelines Clearinghouse (www.guideline.gov), Clinical Evidence (www.clinicalevidence.bmj.com), Intute (www.intute.ac.uk), National Institute for Clinical Excellence (www.nice.org.uk), and other Web sites with similar terms. Inclusion of CPGs was determined by two of the authors (S.D. and A.C.T.) who independently screened the literature search results using predefined relevance criteria. Conflicts were resolved by discussion until consensus was reached.
In order to be eligible, all CPGs had to be related to the management of nonspecific, chronic LBP, had to discuss the evidence supporting both primary care and secondary care interventions, be written in English, regardless of country of conduct or publication status, and based on literature searches that extended within 3 yr of preparing this article (October 2009). Data were abstracted by one author (S.D.) and verified independently by another author (A.C.T.). Dichotomized recommendations pertaining to various primary care and secondary care interventions for managing chronic LBP were abstracted, and the results were summarized descriptively. The methodological and reporting quality of CPGs was assessed using the AGREE instrument to determine whether they were of generally higher or lower quality. [4] Additional information about specific interventions recommended in CPGs was obtained from the previously mentioned January/February 2008 special focus issue of The Spine Journal.
RESULTS
The search uncovered two CPGs that met the eligibility criteria, which were published in three reports. [14, 15, 39] These CPGs were conducted in the United Kingdom [19] and the United States [14, 15] and endorsed by a national government agency [39] or professional medical groups. [14, 15] The CPG from the United States was published in two sections: the first in 2007 was related to primary care interventions [15], and the second in 2009 related to secondary care interventions. [14] Although CPGs from both the United States and the United Kingdom discussed both acute and chronic LBP, setting the threshold for the transition at either 4-12 wk [14, 15] or 6 wk [39], only recommendations concerning chronic LBP are summarized in this article.
Both CPGs were deemed to be of higher methodological quality according to the AGREE instrument. The CPG from the United Kingdom searched the literature through July 2008 and was published in May 2009. [39] The team of authors for this CPG included chiropractors, clinical researchers, general practitioners, general spine specialists, occupational therapists, physical therapists, surgical spine specialist, and systematic review methodologists.
The CPG from the United States related to primary care interventions searched the literature through November 2006 and was published in October 2007. [15] This portion of the U.S. CPG was authored by clinical researchers, general practitioners, general spine specialists, and surgical spine specialists on behalf of a larger CPG steering committee (U.S. primary care). The quality of this portion of the CPG could have been higher if it had included a strategy for updating and descriptions of organizational barriers to implementing the recommendations.

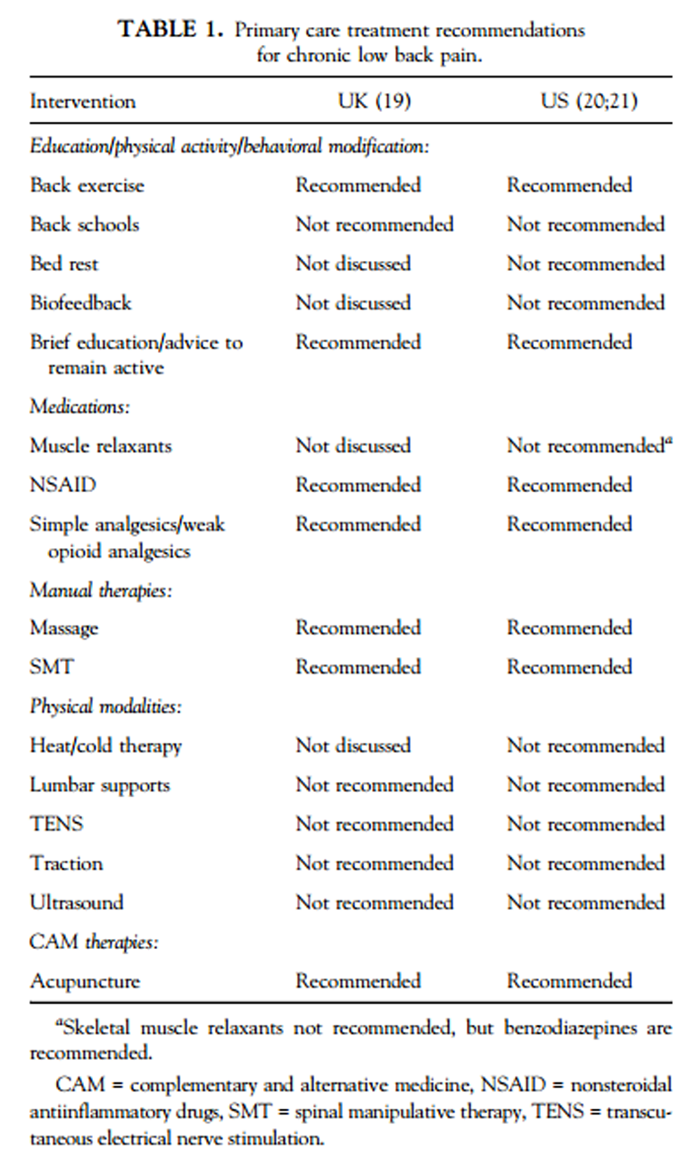
Table 1
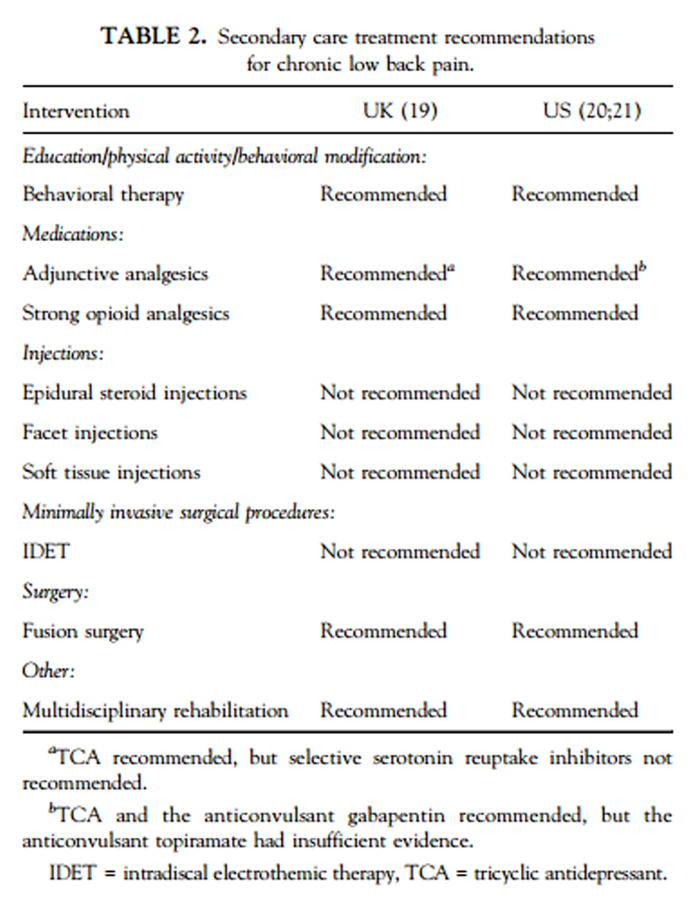
Table 2 The CPG from the United States related to secondary care interventions searched the literature through July 2008 and was published in May 2009. [14] This CPG was authored by general practitioners, general spine specialists, surgical spine specialists, and chiropractors, on behalf of a larger CPG steering committee. Recommendations for the management of chronic LBP from these CPGs are described later in this article and summarized for both primary care (Table 1) and secondary care (Table 2) interventions.
Primary Care Interventions
Some of the primary care interventions recommended by these CPGs included education, analgesics, spinal manipulative therapy (SMT), acupuncture, and exercise. Each is briefly discussed here.
Education
Education about LBP should consist of short interactions with a health provider or lay group discussions, educational booklets, electronic materials, or Web-based discussion groups. [1] The purpose of brief education about LBP generally is to reassure patients about the diagnosis of LBP, inform them about their prognosis, encourage self-care, and provide advice to remain physically active despite any discomfort or pain. [8]
Brief education about LBP should emphasize the following points:1) LBP is very common,
2) LBP rarely is caused by serious pathology,
3) serious pathology related to LBP can be screened effectively by identifying red flags,
4) in 95% of cases of LBP, the location of the specific source of pain cannot be identified,
5) diagnostic testing rarely is helpful and often shows findings that are not relevant to the pain,
6) most LBP gets better within a month, but pain may not disappear completely,
7) recurrence is common,
8) the amount of pain does not indicate that tissues are damaged,
9) it is best to remain physically active despite the pain, and
10) bed rest will likely prolong LBP.
Analgesics
There are numerous types of analgesics available for chronic LBP, including acetaminophen and nonsteroidal antiinflammatory drugs (NSAID), which are some of the most commonly prescribed drugs in the world. [29, 49] Acetaminophen generally is recommended as the first-line medication for chronic LBP, with NSAID as the second-line medication if acetaminophen is ineffective or contraindicated. The combination of acetaminophen and NSAID also is recommended if neither alone is sufficient to reduce symptoms. One advantage to acetaminophen and NSAID is that they generally are available as over-the-counter (OTC) medications, which reduces cost and is conducive to self-care. Should neither prove effective, weak opioid analgesics such as codeine or tramadol may be used on a short-term basis for temporary increases in pain. Use of analgesics must be evaluated against known or potential harms, which include hepatic toxicity with acetaminophen and renal, gastrointestinal, and cardiovascular complications with NSAID (32). Current evidence suggests that there is no difference in the efficacy of specific NSAID, including selective COX-2 inhibitors, and no difference between lower doses and higher doses. Weak opioid analgesics appear only marginally more effective than acetaminophen or NSAID.
Spinal manipulative therapy
High-velocity, low-amplitude (HVLA) SMT involves applying a manual thrust to spinal joints slightly beyond their passive ranges of motion, whereas mobilization involves application of manual force without thrusting. [23] SMT is administered by several groups of trained practitioners, including chiropractors, osteopathic physicians, and physical therapists. The majority (94%) of SMT in the United States is delivered by chiropractors. [45] Several mechanisms of action have been proposed for SMT, including altering the position of anatomic structures, releasing entrapped structures, disrupting soft tissue adhesions, and impacting primary afferent neurons from paraspinal tissues to improve motor control and pain processing. [6] The ideal patient for SMT is a person without red flags (e.g., fracture or trauma, infection, tumor, or systemic inflammation causing tissue disruption to the area being considered for treatment) or severe osteoporosis. The dose of SMT required for clinical improvements for the treatment of chronic LBP is unclear. The UK CPG [39] recommended a maximum dose of nine SMT sessions over a period of up to 12 wk. However, studies have reported that three to four sessions of SMT each week for 3 wk may result in greater short-term pain relief and disability reduction. [21]
Needle acupuncture
Needle acupuncture involves stimulation of anatomical points by penetrating the skin with solid metallic needles that are manually or electrically stimulated. [3] Acupuncture originated in China over 2000 yr ago and consists of many subtypes with distinct characteristics. Whereas the mechanism of action for acupuncture is uncertain, historical theories purport that health is maintained by a balance of "yin" and "yang," and acupuncture assists in maintaining or correcting this balance. [3] Modern theories suggest that acupuncture may achieve relief through counter-irritation or central nervous system stimulation. Acupuncture treatment is administered by licensed acupuncturists and other credentialed providers (e.g., traditional Chinese medicine practitioners, physicians, chiropractors, physiotherapists). In a typical treatment for chronic LBP, approximately 20-30 needles are applied to the skin along meridians (vital energy pathways in the body) and associated acupuncture points and left in place for 20-30 min. The UK CPG [39] recommended a maximum dose of nine acupuncture sessions over a period of up to 12 wk. The ideal patient for acupuncture is someone without contraindications, such as hemophilia, bleeding disorders, needle phobia, cellulitis, local skin infections, or loss of skin integrity. [3]
Exercise
Back exercises generally are recommended for chronic LBP, but differing conclusions have been reached regarding the efficacy and equivalence of specific types of exercise. [17, 25, 31, 46] This partly is because of poor reporting, as studies related to exercise therapy often fail to provide sufficient details on the mode of exercise administered and the protocol followed, such as the dose, duration, and intensity. [35] Conclusions drawn from CPGs about the efficacy of back exercises often overlook the relative efficacy of one specific type of back exercise over another. Two common back exercise approaches to chronic LBP are discussed here.
Back strengthening exercise
Back strengthening exercises are defined as supervised, dynamic, progressive resistance exercises (PRE) with isolation of lumbar extensor muscles. [35] Modes of administration for this form of exercise include machines, benches, Roman chairs, free weights, floor exercises, and stability ball exercises. Strengthening exercises typically are supervised by trained personnel in rehabilitation clinics or fitness centers. Strengthening exercise programs are grounded in the principles of exercise prescription guidelines for muscular strength development [2], such as one to three sets of exercise per session, up to 25 repetitions per set, with one to three training sessions each week. Strengthening exercise is performed throughout the full, pain-free range of motion of back extension, while exercise load gradually and progressively is increased via weight stacks, metal plates, machine angle, or hand position. Back strengthening exercise usually is performed at a higher intensity than other forms of exercises that have been advocated for chronic LBP. The proposed mechanism of actions for back strengthening exercise is that isolated dynamic PRE improves the structural integrity of the affected region, enhances metabolic exchange of lumbar discs, and improves kinesiophobia and locus of control. [26, 37, 43] Other than a thorough physical examination to rule out red flags, no specific diagnostic tests are required to initiate this treatment. The ideal patient for this treatment includes those without cardiovascular or orthopedic contraindications to resistance exercise, those who are willing to take responsibility for their own self-care through active exercise, and those who recognize the potential for long-term benefit, despite possibility of short-term discomfort. [35]
Lumbar stabilization exercise
Lumbar stabilization (i.e., core stabilization) exercises are aimed at improving neuromuscular control, strength, and endurance of muscles in order to maintain dynamic spinal stability by targeting the specific intrinsic muscles of the lower trunk region (e.g., multifidus, transverse abdominis, quadratus lumborum). [48] In contrast to strengthening exercises, stabilization exercises typically are performed isometzrically or within a small range of motion near the neutral trunk position. [36, 42] These exercises are performed on the floor or using stability balls, without external loads, at a low intensity and with minimal progression of resistance. Stabilization exercises initially are supervised by trained personnel, transitioning to unsupervised home exercise during the latter stages. The proposed mechanism of action for stabilization exercise is that training co-contraction of the intrinsic lower trunk muscles enhances spinal stability and facilitates motor control of these muscles by improving firing patterns during functional activities. [48] A patient who exhibits reproducible, mechanical patterns of lumbopelvic pain that follows a specific plane of movement or functional task is an ideal candidate for this treatment. [48]
Secondary Care Interventions
Some of the secondary care interventions recommended by these CPGs include behavioral therapy, multidisciplinary rehabilitation, adjunctive analgesics, strong opioid analgesics, and fusion surgery. Each is briefly discussed here.
Behavioral therapy
Behavioral therapy includes group therapy, psychoanalysis, and cognitive behavioral therapy (CBT), among others. Of these, CBT generally is the most commonly recommended approach for chronic LBP. [19] The goal of CBT is to overcome barriers to recovery by identifying them, and developing strategies to promote self-management and self-efficacy. [19] In the United States, CBT is administered by licensed mental health professionals, including psychologists and psychiatrists. Ideal candidates for this treatment are those who exhibit psychosocial risk factors for chronicity, including anxiety, depression, symptom magnification, and inappropriate expectations. CBT is most effective when combined with other therapies, such as exercise training. [19]
Multidisciplinary rehabilitation
Although multidisciplinary rehabilitation programs vary widely, most consist of the following components: physical, behavioral, vocational, and pharmacologic management. Usually, multidisciplinary rehabilitation is delivered by at least three healthcare providers with different clinical backgrounds, combining intensive supervised exercise therapy with behavioral approaches to decrease pain, improve function, reduce the impact of psychological comorbidities, and foster a return to normal activities for patients with chronic LBP. [20] Numerous specific approaches have been developed within the field of multidisciplinary rehabilitation, which can be thought of as a coordinated, combined approach rather than a specific intervention. The ideal candidate for multidisciplinary rehabilitation is one with severe or prolonged symptoms, psychological comorbidities, few or no contraindications to exercise, and motivation to continue with the program, regardless of temporary muscle soreness.
Adjunctive analgesics
Adjunctive analgesics include tricyclic antidepressants (TCA), selective serotonin reuptake inhibitors (SSRI), serotonin-norepinephrine reuptake inhibitors (SNRI), and antiepileptic drugs. Of these, only TCA was recommended by the CPG. [15, 39] Commonly prescribed TCA include amitriptyline, desipramine, and nortriptyline. [12] TCA generally are recommended as the fourth-line medication for LBP if acetaminophen, NSAID, and weak opioids do not provide adequate relief of symptoms. [12] TCA can be used if symptoms of depression are present, but some patients will experience moderate pain relief regardless of their depression status. Some TCA also may be useful for patients with chronic LBP and sleep disturbances. The use of TCA should be balanced with harms that can occur, such as dry mouth and nose, blurred vision, constipation, urinary retention, memory difficulties, drowsiness, restlessness, dizziness, weight gain, sweating, decrease in sexual ability and desire, nausea, vomiting, seizures, and coma. [12] These side effects may worsen as the dosage increases. [12]
Strong opioid analgesics
Strong opioid analgesics generally are not recommended as first-line medications for chronic LBP, but can be considered for severe, disabling symptoms that cannot be managed adequately through acetaminophen, NSAID, weak opioids, and nonpharmacologic approaches. [44] Strong opioid analgesics include morphine, oxycodone, fentanyl, and methadone. It is recommended that these medications should be prescribed by pain management specialists with the necessary training for titrating the dosage and monitoring patients for signs of addiction, dependency, compliance, and deviant behaviors. [44] The use of these medications needs to be balanced by their potential side effects, including risk of dependency, headache, constipation, vomiting, nausea, dry mouth, dizziness, drowsiness, decrease in sexual ability and desire, sweating, peripheral edema, and respiratory depression. Strong opioid analgesics only should be used on a limited basis.
Fusion surgery
For chronic LBP that is associated with severe degenerative changes such as advanced spondylolisthesis, spinal stenosis, and documented instability, surgical fusion may be appropriate. [16] Traditional fusion surgery generally involves removing damaged intervertebral discs, and placing autograft bone chips taken from the iliac crest between the vertebrae to help them fuse. [16] Several variations on fusion surgery also are available, including allograft using bone morphogenic protein (BMP) and use of metal instrumentation such as pedicle screws or interbody cages to further secure the fused vertebrae. Arthroplasty, which involves removing the intervertebral disc and replacing it with a device that allows movement (often termed an artificial disc), recently has been proposed as an alternative to traditional fusion surgery. [16] At this time, available research suggests that there are no significant differences in outcome between the different surgical techniques. [14] Fusion surgery or arthroplasty in patients with high fear avoidance of pain, psychological distress, loss of work, compensation claims, personal injury litigation, and job dissatisfaction should be considered with care as these characteristics predict poorer outcomes. [10, 16] If fusion is being considered for chronic LBP without serious pathology, clinicians should inform patients that intensive multi-disciplinary rehabilitation might produce the same outcome. [7]
DISCUSSION
Based on the reviewed CPGs, an evidence-informed approach to the management of chronic LBP would begin with a thorough history and physical examination to rule out serious spinal pathology, nonspinal causes, and severe or progressive neurologic deficits. For the majority of patients with nonspecific, chronic LBP, first-line approaches would center on self-care, brief education, and acetaminophen or NSAID. [15] For patients whose symptoms do not resolve with these approaches, incorporation of back strengthening or stabilization exercises is recommended to achieve long-term improvements in function. For short-term relief of symptoms, limited trials of SMT or acupuncture also are recommended. [15]
Several commonly used primary care approaches were not recommended by recent CPGs for chronic LBP, including bed rest, biofeedback, lumbar supports, muscle relaxants, and physical modalities such as heat, cold, traction, transcutaneous electrical nerve stimulation (TENS), and ultrasound. Although each of these interventions is based on a purported mechanism of action that may be plausible, evidence suggests that they do not produce meaningful clinical improvement despite a long history of use. The concept of relying exclusively on devices, machines, or other equipment to temporarily relieve or even eliminate chronic LBP is appealing, but evidence suggests that active participation by the patient is the most essential element for the control of or recovery from chronic LBP.
Only a few secondary care interventions were recommended by recent CPGs, including behavioral therapy, multidisciplinary rehabilitation, adjunctive analgesics, strong opioid analgesics, and fusion surgery. It should be noted, however, that even when CPGs recommended these interventions for chronic LBP, there were caveats about specific indications. For example, behavioral therapy was recommended for patients with chronic LBP and psychological comorbidities such as anxiety, depression, or fear avoidance behavior. Similarly, only a few adjunctive analgesics were recommended in those patients with specific comorbidities. Fusion surgery was recommended primarily for severe symptoms associated with specific anatomical diagnoses such as spondylolisthesis, stenosis or instability. These recommendations therefore should not be construed as broad endorsements for all patients with chronic LBP.
Many other commonly used secondary care interventions, including all forms of injections and minimally invasive intradiscal approaches, and other forms of surgical interventions, were not recommended for the management of chronic LBP without radiculopathy. [14, 15, 39] These interventions typically target specific anatomical structures. Unfortunately, current research suggests that there is considerable difficulty and no consensus as to whether it is possible to establish an anatomical basis for the vast majority of patients with nonspecific, chronic LBP. Hopefully in the future, advances in the understanding of the etiology of chronic LBP will help guide the appropriate use, if any, of interventions aimed at specific anatomical structures.
CONCLUSION
The evidence from current CPGs and other significant reviews indicates that the primary care management of chronic LBP should start with a thorough history and physical exam to screen for red flags to rule out serious pathologies. In the absence of red flags, treatment initially should focus on self-care and brief education, along with NSAID or simple analgesic medications for short-term pain relief. For patients whose symptoms do not resolve with first-line approaches, back exercises to address functional deficits, and SMT, massage, or acupuncture for pain relief are recommended. For patients with chronic LBP who exhibit psychological comorbidities, adjunctive analgesics, behavioral therapy, or multidisciplinary rehabilitation may be appropriate.
Given the uncertainty about which treatment approach is most effective, patient preference should be solicited in this decision-making process since expectations likely will impact the long-term outcomes.
References:
Airaksinen O, Brox JI, Cedraschi C, et al.
COST B13 Working Group on Guidelines for Chronic Low Back Pain Chapter 4.
European Guidelines for the Management of Chronic Nonspecific Low Back Pain
European Spine Journal 2006 (Mar); 15 Suppl 2: S192–300
See also the archived: European Guidelines Backpain Europe WebsiteAmerican College of Sports Medicine.
ACSM's Guidelines for Exercise Testing and Prescription.
New York: Lippincott Williams & Wilkins; 2010.Ammendolia C, Furlan AD, Imamura M, et al.
Evidence-informed management of chronic low back pain
with needle acupuncture.
Spine J. 2008; 8:160-72.Appraisal of Guidelines Research and Evaluation
in Europe Collaborative Group.
Guideline development in Europe.
An international comparison.
Int. J. Technol. Assess. Health Care. 2000; 16:1039-49.Bennett GG, Wolin KY, Puleo EM, et al.
Awareness of national physical activity recommendations
for health promotion among US adults.
Med. Sci. Sports Exerc. 2009; 41:1849-55.Bronfort, G, Haas, M, Evans, R, Kawchuk, G, and Dagenais, S.
Evidence-informed Management of Chronic Low Back Pain
with Spinal Manipulation and Mobilization
Spine J. 2008 (Jan); 8 (1): 213–225Brox JI, Sorensen R, Friis A, et al.
Randomized clinical trial of lumbar instrumented fusion
and cognitive intervention and exercises in patients
with chronic low back pain and disc degeneration.
Spine. 2003; 28:1913-21.Brox JI, Storheim K, Grotle M, et al.
Evidence-informed management of chronic low back pain
with back schools, brief education, and
fear-avoidance training.
Spine J. 2008; 8:28-39.Carlson C.
Axial back pain in the athlete:
pathophysiology and approach to rehabilitation. Curr.
Rev. Musculoskelet. Med. 2009; 2:88-93.Carragee EJ, Alamin TF, Miller JL, et al.
Discographic, MRI and psychosocial determinants of low back pain
disability and remission: a prospective study in subjects
with benign persistent back pain.
Spine J. 2005; 5:24-35.Cassidy JD, Cote P, Carroll LJ, Kristman V.
Incidence and course of low back pain episodes in the
general population.
Spine. 2005; 30:2817-23.Chang V, Gonzalez P, Akuthota V.
Evidence-informed management of chronic low back pain
with adjunctive analgesics.
Spine J. 2008; 8:21-7.Chen SM, Liu MF, Cook J, et al.
Sedentary lifestyle as a risk factor for low back pain:
a systematic review.
Int. Arch. Occup. Environ. Health. 2009; 82:797-806.Chou R, Loeser JD, Owens DK, Rosenquist RW, Atlas SJ, Baisden J, et al.
Interventional Therapies, Surgery, and Interdisciplinary Rehabilitation for Low Back Pain:
An Evidence-based Clinical Practice Guideline From the American Pain Society
Spine (Phila Pa 1976). 2009 (May 1); 34 (10): 1066–1077Chou R, Qaseem A, Snow V, Casey D, Cross JT Jr., Shekelle P, Owens DK:
Diagnosis and Treatment of Low Back Pain: A Joint Clinical Practice Guideline
from the American College of Physicians and the American Pain Society
Annals of Internal Medicine 2007 (Oct 2); 147 (7): 478–491Don AS, Carragee E.
A brief overview of evidence-informed management of
chronic low back pain with surgery.
Spine J. 2008; 8:258-65.Ferreira PH, Ferreira ML, Maher CG, Herbert RD, Refshauge K.
Specific stabilisation exercise for spinal and pelvic pain:
a systematic review.
Aust. J. Physiother. 2006; 52:79-88.Frymoyer JW, Cats-Baril WL.
An overview of the incidences and costs of low back pain.
Orthop. Clin. North Am. 1991; 22:263-71.Gatchel RJ, Rollings KH.
Evidence-informed management of chronic low back pain
with cognitive behavioral therapy.
Spine J. 2008; 8:40-4.Guzman J, Esmail R, Karjalainen K, et al.
Multidisciplinary rehabilitation for chronic low back pain:
systematic review.
BMJ. 2001; 322:1511-6.Haas, M., Groupp, E., and Kraemer, D.F.
Dose-response for Chiropractic Care of Chronic Low Back Pain
Spine J 2004 (Sep); 4 (5): 574–583Haldeman S, Dagenais S.
A Supermarket Approach to the Evidence-informed Management of Chronic Low Back Pain
Spine Journal 2008 (Jan); 8 (1): 1–7Haldeman S, Phillips RB, Frymoyer JW, et al.
Spinal manipulative therapy in the management of low back pain.
In: The Adult Spine: Principles and Practice.
New York: Raven Press; 1991, p. 1581-605.Haskell WL, Lee IM, Pate RR, et al.
Physical activity and public health: updated recommendation
for adults from the American College of Sports Medicine
and the American Heart Association.
Med. Sci. Sports Exerc. 2007; 39:1423-34.Hayden JA, van Tulder MW, Malmivaara A, Koes BW.
Exercise therapy for treatment of non-specific low back pain.
Cochrane Database Syst. Rev. 2005(3):CD000335.Helmhout PH, Harts CC, Staal JB, et al.
Comparison of a high-intensity and a low-intensity
lumbar extensor training program as minimal intervention
treatment in low back pain: a randomized trial.
Eur. Spine J. 2004; 13:537-47.Heneweer H, Vanhees L, Picavet HS.
Physical activity and low back pain: a u-shaped relation?
Pain. 2009; 143:21-5.Iwai K, Nakazato K, Irie K, et al.
Trunk muscle strength and disability level of low back pain
in collegiate wrestlers.
Med. Sci. Sports Exerc. 2004; 36:1296-300.Koes BW, Scholten RJ, Mens JM, Bouter LM.
Efficacy of non-steroidal anti-inflammatory drugs for low back
pain: a systematic review of randomised clinical trials.
Ann. Rheum. Dis. 1997; 56:214-23.Levangie PK.
Association of low back pain with self-reported risk factors
among patients seeking physical therapy services.
Phys Ther. 1999; 79:757-66.Liddle SD, Baxter GD, Gracey JH.
Exercise and chronic low back pain: what works?
Pain. 2004; 107:176-90.Malanga G, Wolff E.
Evidence-informed management of chronic low back pain
with nonsteroidal anti-inflammatory drugs, muscle relaxants,
and simple analgesics.
Spine J. 2008; 8:173-84.Manchikanti L, Singh V, Datta S, et al.
Comprehensive review of epidemiology, scope, and impact
of spinal pain.
Pain Physician. 2009; 12:E35-70.Martin, BI, Deyo, RA, Mirza, SK et al.
Expenditures and Health Status Among Adults With Back and Neck Problems
JAMA 2008 (Feb 13); 299 (6): 656–664Bronfort, G, Haas, M, Evans, R, Kawchuk, G, and Dagenais, S.
Evidence-informed Management of Chronic Low Back Pain
with Spinal Manipulation and Mobilization
Spine J. 2008 (Jan); 8 (1): 213–225McGill SM.
Low back exercises: evidence for improving exercise regimens.
Phys. Ther. 1998; 78:754-65.Mooney V, Verna JL, Morris CE.
Clinical management of chronic, disabling low back syndromes.
In: Low Back Syndromes:
Integrated Clinical Management,
New York: McGraw-Hill; 2006.Nadler SF, Wu KD, Galski T, Feinberg JH.
Low back pain in college athletes. A prospective study
correlating lower extremity overuse or acquired
ligamentous laxity with low back pain.
Spine. 1998; 23:828-33.National Institute for Health and Clinical Excellence (NICE).
Low Back Pain: Early Management of Persistent Nonspecific Low Back Pain
London: National Institute for Health and Care Excellence; 2009.
[Report No.: Clinical guideline 88].Pengel LH, Herbert RD, Maher CG, Refshauge KM.
Acute low back pain: systematic review of its prognosis.
BMJ. 2003; 327:323.Quebec Task Force on Spinal Disorders.
Scientific approach to the assessment and management of
activity-related spinal disorders. A monograph for clinicians.
Report of the Quebec Task Force on Spinal Disorders.
Spine. 1987; 12(Suppl. 7):S1-59.Richardson C, Jull G, Hodges P, Hides J.
Therapeutic Exercise for Spinal Segmental Stabilization
in Low Back Pain.
Edinburgh, Scotland:
Churchill Livingstone; 1999.Risch S, Norvell N, Pollock M, et al.
Lumbar strengthening in chronic low back pain patients.
Physiologic and psychological benefits.
Spine. 1993; 18:232-38.Schofferman J, Mazanec D.
Evidence-informed management of chronic low back pain with
opioid analgesics.
Spine J. 2008; 8:185-94.Shekelle PG, Adams AH, Chassin MR, et al.
Spinal manipulation for low-back pain.
Ann. Intern. Med. 1992; 117:590-8.Smeets RJ, Wade D, Hidding A, et al.
The association of physical deconditioning and chronic low back pain:
a hypothesis-oriented systematic review.
Disabil. Rehabil. 2006; 28:673-93.Standaert CJ, Herring SA, Pratt TW.
Rehabilitation of the athlete with low back pain.
Curr. Sports Med. Rep. 2004; 3:35-40.Standaert CJ, Weinstein SM, Rumpeltes J.
Evidence-informed management of chronic low back pain with
lumbar stabilization exercises.
Spine J. 2008; 8:114-20.van Tulder MW, Scholten RJ, Koes BW, Deyo RA.
Nonsteroidal anti-inflammatory drugs for low back pain:
a systematic review within the framework of the
Cochrane Collaboration Back Review Group.
Spine. 2000; 25:2501-13.Von Korff M, Saunders K.
The course of back pain in primary care.
Spine. 1996; 21:2833-7
Return to LOW BACK PAIN
Since 2-15-2010
| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |