

Adverse Events Among Older Adults Receiving Chiropractic
Spinal Manipulation and Related Treatments:
An Updated Systematic Review
This section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: Chiropractic & Manual Therapies 2026 (Mar 16); 34: 15 ~ FULL TEXT
OPEN ACCESS Clinton J. Daniels • Ronald J. Farabaugh • Stacie A. Salsbury • Kristian R. Anderson • Maranda J Kleppe • Wayne M. Whalen • Sheryl A. Walters • Lisa Z. Killinger • Alec L. Schielke
VA Puget Sound Health Care System,
9600 Veterans Drive SW,
Tacoma, WA, USA.
Background This systematic review updated adverse events (AEs) reporting in persons aged > 55 years who received chiropractic treatment, including spinal manipulation.
Methods Protocol was registered prospectively with the Prospective Register of Systematic Reviews (PROSPERO)(CRD42024629286). Search strategy was audited with Peer Review of Electronic Search Strategies (PRESS) methodology. We searched PubMed, Cochrane Central Register of Controlled Trials, CINAHL, AMED, and Index to Chiropractic Literature on December 12, 2025. We included AEs attributed to treatment provided by chiropractors reported in randomized clinical trials (RCTs), observational studies, and case reports/series. We excluded non-clinical, pilot/feasibility studies, surveys, reviews, populations ≤ 55 years,and papers lacking chiropractic treatment or AE descriptions. Articles were screened and results synthesized by study design and AE characteristics. Study risk of bias (RoB) was assessed in duplicate using Scottish Intercollegiate Guideline Network checklists. Clinical Compass and NCMIC Foundation partially funded this study.
Results We screened 2295 titles/abstracts, reviewed 125 full-text, and included 25 articles from 6 RCTs, 4 observational studies, and 15 case reports/series. One RCT had low RoB and five acceptable. Three observational cohorts had low RoB and 1 had acceptable. There were 412 study-related adverse events affecting older adult patients, of which 9 were severe, and none were catastrophic. Most adverse events were rated as mild-to-moderate in severity. Reported adverse events consisted of changes in pain quality, muscle or joint soreness or stiffness, numbness, weakness, fatigue, headache, dizziness, or lightheadedness. Several studies lacked AE definitions and/or data collection processes. Case reports described 6 severe AEs; four were vascular in nature. Twenty case reports involved spinal manipulation, one followed TENS application, and one repetitive shoulder abduction, while no case reports described AEs following chiropractor treatment with soft tissue techniques, exercise, or other modalities.
Conclusion No catastrophic AEs were reported in older adults receiving chiropractic treatment services. Mild-to-moderate symptoms such as muscle soreness and stiffness were common. The lack of standardized AE definitions, severity classifications, and data collection processes across reports limits the certainty. Notable study limitations included a search strategy focused on spinal manipulation, exclusion of administrative database studies that may detect rare AEs, and numerical scoring of RoB checklists.
From the FULL TEXT Article:
Background
Patient safety is high priority for chiropractors, especially those treating older adults with musculoskeletal conditions. [1–3] Musculoskeletal pain conditions are common among older adults. [4] Low back and neck pain are the most common conditions seen by chiropractors [5, 6], have the highest prevalence in older adults [7, 8], and age-adjusted disability related to osteoarthritis is on the rise. [9, 10] In addition to age-related changes, high rates of physical, psychosocial, and social factors further complicate the chronic pain presentation for older adults. [11] The odds of spinal pain in older adults increase with subsequent number of comorbidities [12], and spinal pain may precipitate cognitive impairment. [13] Older adults with spinal pain require careful attention during evaluation and diagnosis as serious pathology is not uncommon in this patient group. [14, 15]
To manage their musculoskeletal complaints, older adults often use nonpharmacologic therapies provided by chiropractors (e.g., spinal manipulation, exercise, manual therapy modalities). [16] Spinal manipulation therapy (SMT) is a nonpharmacologic manual therapy approach that is recommended by medical guidelines for both acute and chronic low back pain (LBP). [17, 18] Older adults who initially use SMT for an episode of chronic LBP have lower rates of care escalation compared to those who use opioid medications as a first treatment. [19] SMT and other manual therapies appear to be well-tolerated and have demonstratable safety profiles in the older adult population. [20] For example, Whedon and associates (2015) reported that older Medicare beneficiaries who received chiropractic treatment had a cumulative probability of injury of 40 incidents per 100,000 patients, which was lower than the 153 injuries per 100,000 patients who had primary care encounters.
However, injuries were more common among older chiropractic patients with coagulation problems and those taking anticoagulation treatments, and people with osteoporosis, aortic aneurysm or dissection, and inflammatory spondylopathies. [21] Prevalent comorbidities in older adults, such as frailty [22], fall risk [23], osteoporosis [24, 25], cancer [21], chronic anticoagulant medication use [21, 26], and history of stroke [21, 26] may put patients at higher risk of adverse events (AEs) or be a contraindication to SMT treatment. [25]
Adverse events are understood as unfavorable events occurring following interventions, but there is no commonly accepted definition of what qualifies as an AE relative to spinal and peripheral joint manipulation and mobilization. [27] Severity classifications of AEs remain controversial despite efforts to establish consensus terminology. [28–30] Approximately half of chiropractic patients experience AEs (e.g., muscle soreness and stiffness) of mild-to-moderate severity and transient nature following SMT. [31] Further, in the presence of comorbidities, SMT is associated with rare and consequential AEs that may have significant impact on a patient’s wellbeing, function, and quality of life, such as fracture in the presence of osteoporosis, dislocation in the presence of inflammatory spondylopathy, brain or spinal cord injury when using long-term anticoagulant therapy, and cervical artery dissection. [ 21, 31, 32]
A 2010 systematic review and consensus study, initially updated in 2017, evaluated the safety of chiropractic care for the older adult population and found that a higher rate of AEs were not associated with high-velocity, low-amplitude SMT as compared to low-velocity, low-amplitude SMT or sham. [33, 34] That 2017 update included six papers relevant to adverse events: an RCT [35], an RCT pilot [36], a case series [37], two cohorts of claims data [21, 38], and a narrative review. [39]
The prior review did not find any studies on non-SMT treatments offered by chiropractors (e.g., exercise, modalities, advice), and they identified the need to further investigate the safety of managing older adults. Since the prior review, research interest in chiropractic care of the older adult population has led to numerous publications. [40, 41] In addition, the World Federation of Chiropractic has called on the chiropractic profession to actively engage in the advancement of patient safety. [42] Therefore, the purpose of this review was to provide an update on the safety literature on AEs in older adults following chiropractic treatment sessions that included spinal manipulation. Further, the results of this review will inform an updated consensus process on chiropractic management of older adults.
Methods
Registration and protocol
The protocol was prospectively registered with the International Prospective Register of Systematic Reviews (PROSPERO) on December 19, 2024 (CRD42024629286). [43] Study reporting was consistent with the Preferred Reporting of Systematic Reviews and Meta-Analysis (PRISMA). [44]
Eligibility criteria

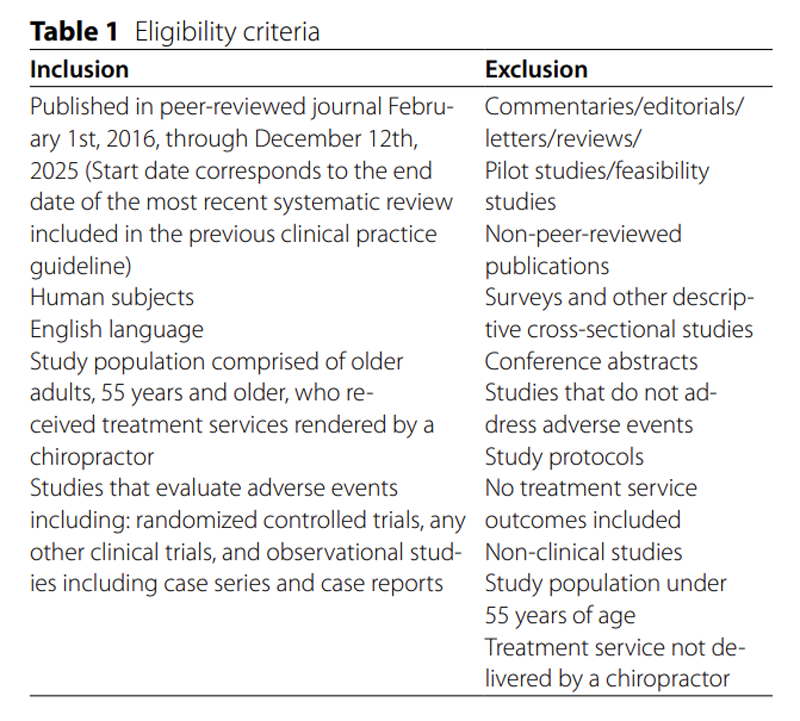
Table 1 The study aim was processed into PICOS (population, intervention, comparison, outcomes, and study design) components to develop eligibility criteria (Table 1).
Population
The prior systematic review by Hawk et. al defined older adults as 65 and older, however, they included an RCT that enrolled participants aged ≥55 years old [mean (SD) age 64.5 (8.9) years]. [45] In this updated systematic review, an a priori decision was made to define older adults as 55 years and over for consistency with Hawk et al and to maximize the number of eligible studies. This decision was supported by a systematic review of older adults studies inclusion criteria finding a mean age of 61 (SD ±9.2) years [46] and the BACk Complaints in Elders (BACE) cohort study which included participants ≥55 years old. [47–49] We included case reports and clinical studies in which all participants were aged 55 years or older, or observational studies and clinical trials with a mean participant age of approximately 55 years old for which individual data were available.
Intervention
Chiropractic treatments were defined as non-pharmacological interventions delivered by a chiropractor. Spinal manipulative therapy was the primary intervention evaluated, but chiropractic treatments also included, but were not limited to, manual therapy, supervised exercise, mind-body interventions, acupuncture, massage therapy, acupressure, electrical modalities, and the application of heat or cold. Treatments could be used independently or in combination.
Comparison
No comparison was required.
Outcomes
The study or case report was required to provide a description of AEs associated with a chiropractic treatment for inclusion into this review. Adverse events that were deemed by the original study as not-study related were not included. For studies that did not specify if an adverse event was related to the study or external factors, we treated all adverse events reported as study-related. No study level exclusions were made based on whether the authors described the relatedness of AEs to the study.
Study design
We included study designs that addressed AEs including randomized controlled trials and other clinical trials, as well as observational designs, such as cohorts, case series and case reports. This deviated from the 2017 review, which had less restrictive inclusion criteria and included pilot studies, claims data, and narrative reviews.
Information Sources
Databases PubMed, Cochrane Central Register of Controlled Trials, CINAHL (Cumulative Index to Nursing and Allied Health Literature), AMED (Allied and Complementary Medicine Database), and ICL (Index to Chiropractic Literature) were searched from the end of the Hawk et al. study through December 18, 2024. The search was last conducted on December 12, 2025. In addition, adverse event articles from the 2017 review by Hawk et al. were included in the screening for eligibility for this updated review [34], and manual citation tracking was performed on included articles to identify potentially relevant articles.
Search Strategy
The search strategy was designed in collaboration with a health sciences librarian (SAW). A second health science librarian assessed the search strategy with the Peer Review of Electronic Search Strategies (PRESS) checklist (Supplemental File A) and additional revisions were made to generate the full search strategy (Supplemental File B). The search terms focused on treatment approaches employed by chiropractors. For example, the search conducted within PubMed, which generated the most returns, included the keywords “adverse effects” paired with the National Library of Medicine Medical Subject Heading (MeSH) for Musculoskeletal Manipulations, which is the preferred (most general) term to identify publications with the following scope: ‘various manipulations of body tissues, muscles and bones by hands or equipment to improve health and circulation, relieve fatigue, promote healing’. MeSH tree structures under this broader heading also were searched, including Manipulation, Chiropractic; Manipulation, Spinal; Manipulation, Osteopathic; and Manipulation, Orthopedic. The search strategy also gathered citations using patient safety terminology (harm, risk, injury, adverse event, adverse effect, etc.) and specific adverse event categories (fracture, cauda equina or complication, artery dissection, etc.).
Chiropractic search terms searched the databases with the wildcard term “chiropract*” (to capture any article with the terms chiropractic/chiropractor/chiropractics/chiropractors) and variations of spinal manipulation. We did not include a comprehensive list of interventions beyond spinal manipulation (e.g., terms related to exercise, soft tissue therapy, acupuncture, dry needling, or passive modalities) as these are not specific to the chiropractic profession. These interventions were included in the analysis when identified through the chiropractic or spinal manipulation related terms.
Selection Process
Citations identified through database search were downloaded into Rayyan, a web application to support screening for systematic reviews. [50] After duplicates were removed, titles and abstracts were independently screened against the eligibility criteria by at least two reviewers (RF, LK, CD). Full text of the potentially eligible articles were independently screened by two reviewers (RF, CD) and disagreements were resolved through discussion. The citations excluded at this stage were tracked with reason recorded.
Data Collection Process
Data extraction was completed independently by two groups of paired individuals. Two investigators extracted information from case reports and series (KA, WW), and at least two individuals extracted information from RCTs and cohort studies (MK, SS, CD). Differences were adjudicated through discussion and feedback from a third investigator (CD). Corresponding authors were contacted for eleven studies with a request to provide clarification or for AE data for participants 55 years and older, which was provided by seven authors [51–57], one of which did not meet eligibility criteria. [56]
Data Items
Data extracted from eligible RCTs and observational studies included first author surname, publication year, study population, population mean age, sex, condition(s), mean symptom duration, chiropractic treatment group intervention, control group intervention(s), dosage (e.g., number of sessions), AE definition, AE collection method, AEs related to the chiropractic treatment arm(s), and study conclusions. For case reports and series, extraction items included first author surname, publication year, patient age, sex, physical comorbidities, psychological comorbidities, symptoms preceding presentation to the chiropractor, treatment services rendered by the chiropractor, time between treatment and AE occurrence (i.e., 0–2 days, 3–7 days), AE description.
Study risk of bias assessment
Risk of bias assessment was performed on all included articles. RCTs and observational studies were independently assessed by at least two investigators (MK, SS, CD) using the corresponding study design checklist from the Scottish Intercollegiate Guideline Network (SIGN), consistent with the prior review. [58] The SIGN checklist for RCTs is a 10–question assessment, and the cohort checklist is a 14–question assessment. Case reports and series were independently assessed by two investigators (KA,WW) using the JBI Critical Appraisal Checklist for Case Reports. [59] Disagreements for both teams were resolved through discussion and adjudication by a third investigator (CD). Each checklist question was marked as “1” for “yes” or “0” for “no” or “unclear”, or “NA [not applicable]”. The overall risk of bias assessment for all three tools was determined through the percentage of the total score: greater than or equal to 75% were rated as high quality, low risk of bias, between 50% and 75% were rated moderate quality, acceptable risk of bias, and 50% or below was deemed low quality, high risk of bias and excluded. Not applicable items were deducted from the denominator when calculating percentages.
Effect measures
We rated the severity of adverse events described in the studies.
Synthesis Methods
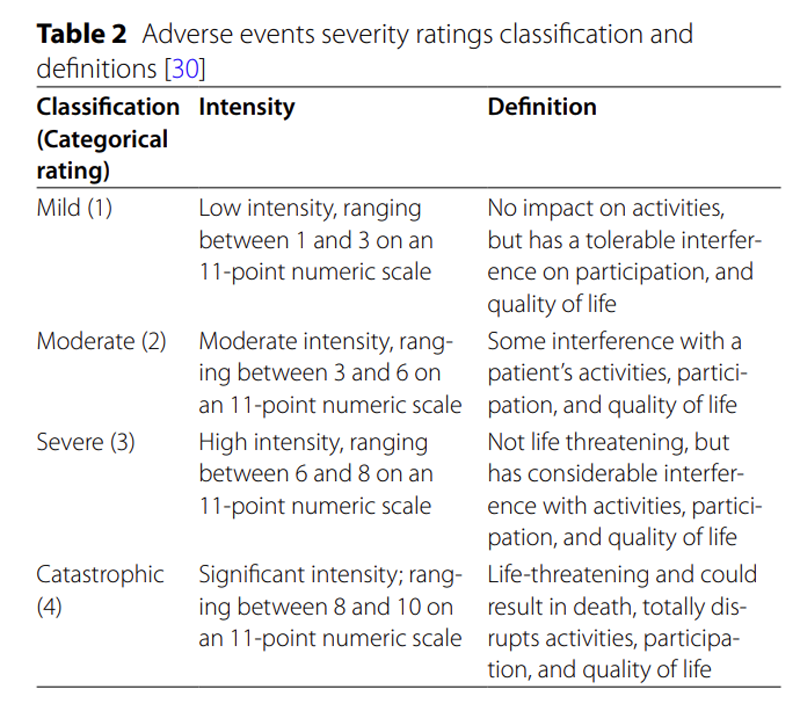
Table 2 We qualitatively synthesized extracted data and organized it by study design, definition of AEs, and AE data collection process. Adverse event severity ratings were classified as 1–4 (1=mild, 2=moderate, 3=severe, 4=catastrophic [life-threatening]) [30] (Table 2). Body system AEs were operationalized as vascular, non-vascular, or both. We also summarized outcomes by type of intervention, quality of studies, and AEs. For the RCTs and cohort studies, we rated the AEs using the descriptions provided in the studies, and for case reports the classification was determined through discussion of the investigators that independently performed extraction (KA, WW, CD).
Reporting biases
Meta-analysis and subgroup analysis were not performed. We investigated reporting biases by comparing definitions and collection processes described in the RCT and observational studies.
Certainty of evidence
Due to the descriptive nature of this systematic review and the wide range of study designs included, we did not assess for certainty.
Results
Study Selection
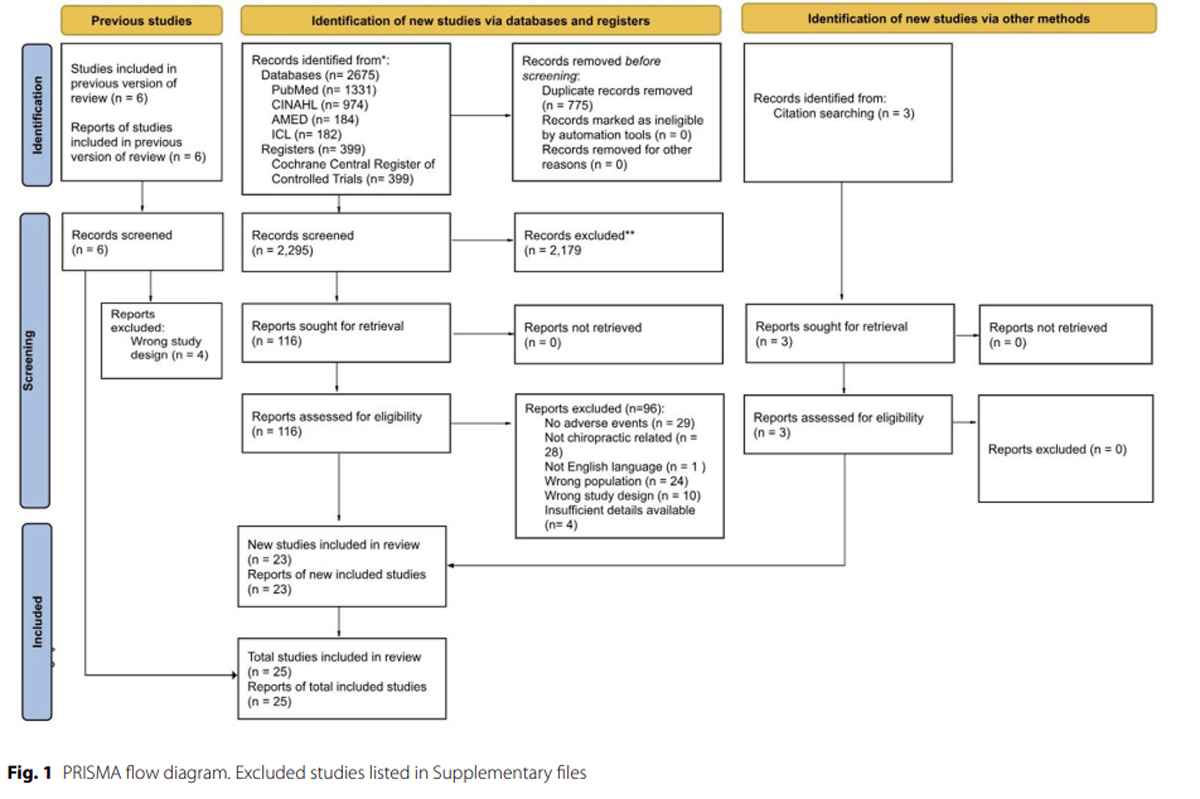
Figure 1 Study investigators screened 2,295 titles/abstracts and 125 full-text articles, of which 25 met the eligibility criteria. The selection process is outlined in Figure 1.
Of the 125 full-text screened articles, 116 were identified from the database and registry search, six were identified from the Hawk et al. 2017 review [34], and an additional three were identified from citation tracking. Ninety-six articles were excluded with reasons provided (Supplemental File C). The most common exclusion reasons were not describing AEs (n = 29), not including an older adult population (n = 24), and describing AEs that did not involve a chiropractor (n = 28). The 25 included articles consisted of six RCTs [35, 53, 54, 60–62], four observational studies [51, 52, 55, 57], and 15 case reports/series [32, 37, 63–75] describing 22 cases.
Study Characteristics
The clinical studies and case series/case reports described 412 adverse events affecting older adult patients related to chiropractic treatment. Most were classified as mild to moderate, eleven were severe, and none were catastrophic. All studies, not exclusively describing severe adverse events, did report mild events (e.g., transient increased pain).
Study design – RCT
Four RCTs investigated chiropractic treatment of older adults with LBP [35, 53, 60, 62], one studied lumbar spinal stenosis [61], and one low back and neck disability. [54] All six RCTs described study-related interventions that included SMT, as well as chiropractic treatments such as mobilization, flexion-distraction, instrument assisted manipulations, soft tissue massage, exercises or self-care recommendations. None of the RCTs reported study-related severe or catastrophic AEs. For patients receiving care for LBP, Bronfort et al. described the most common AEs as patients reporting a different type of pain (n = 16), soreness (n = 17), increased pain (n = 8), leg pain, numbness, weakness (n = 8), fatigue (n = 8), and/or dizziness/lightheadedness (n = 8). [53] Dougherty et al. described 35 AEs definitely/probably associated with the intervention, all of which were mild to moderate soreness, with 42% related to preexisting conditions. [35] Of 414 AEs identified by Goertz et al., 98 were classified as possibly, probably, or definitely related to chiropractic intervention. Of those, seven were rated as moderate severity and 91 mild, with most involving LBP, joint pain, or stiffness. [60] Schulz et al. only collected data on “serious” AEs, and none were determined to be related to the chiropractic treatment arm. [62]
For patients with lumbar spinal stenosis, Schneider et al. reported the most common AEs were characterized as muscle soreness (n = 43) and joint soreness (n = 39), with all AEs resolved within 48 hours. [61] Maiers et al. reported that six older adult patients receiving care for neck and low back disability experienced a combination of symptoms, including increased neck pain (n = 2), back pain (n = 1), numbness in the hands (n = 2) or feet (n = 2), headache (n = 1), and dizziness with exercise (n = 1). [54]
Study design – Observational
One observational study by Pohlman et al. involved active surveillance of AEs in chiropractic and physical therapy clinics in Canada and the United States [55], a second by Chu et al. reported a retrospective study of all reported AEs following receipt of chiropractic SMT in a Hong Kong medical clinic [52], a third by Gliedt et al. performed a retrospective chart-review investigating for serious adverse events in chiropractic patients with prior spine surgery [57], and a fourth study by Amorin-Woods et al. retrospectively searched 15–years of chiropractic student clinics in Western Australia. [51] Pohlman et al. provided individual patient data and we did not include any adverse events encounter in the physical therapy clinics. [55] Amorin-Woods et al., Chu et al., and Gliedt et al. all provided individual-patient data for all patients 55 years and older. [51, 52, 57]
No catastrophic events were reported for the older adult population in any of the observational studies. Out of 54,846 patients, Chu et al. reported 16 older adults with AEs following SMT, most of whom presented for a LBP condition (n = 11), neck pain (n = 3), or an extremity condition (n = 2). Two of the reported AEs were rib fractures, 4 were cases of chest pain without rib fracture, 1 case of jaw pain, and 9 patients with increased pain to the area of chief complaint. Out of 2,136 patients, Pohlman et al. reported 61 older adults experiencing AEs following chiropractic care for LBP (n = 34), neck pain (n = 21), midback pain (n = 17), and/or an extremity condition (n = 26). [55] None of the AEs were described as serious [catastrophic], five were severe and 18 as moderate, with the most common symptoms being discomfort/pain (n = 22), tiredness/fatigue (n = 9), and numbness (n = 9). Gliedt et al reported on 174 older adult patients with prior spine surgery, none of which experienced a serious adverse event. [57] Of 61,882 patients, Amorin-Woods et al. reported only 20 AEs and, of those, only 6 involved patients 55 years and older. The AEs experienced by older adults consisted of increased LBP (n = 4), increased neck pain (n = 1), and dizziness and foot numbness (n = 1), all of which they rated as mild. [51]
Study design – Case reports
Fifteen case reports described AEs purported as associated with chiropractic treatment. One of the cases described an AE of implantable cardioverter defibrillator (ICD) shock following the application of a transcutaneous electrical nerve stimulation (TENS) unit [71], one dislodged a pacemaker lead with repetitive shoulder abduction [68], and the other 20 were attributed to SMT. Three patients were described as presenting to the chiropractor for LBP, three for a combination of neck, midback, and low back, one for hand numbness, six of chronic obstructive pulmonary disease (COPD), and seven did not describe why the patient presented for chiropractic care. None of the case report AEs were catastrophic, but six were severe; of those, four were vascular [dislodged pacemaker lead [68], epidural hematoma [69], vertebral artery dissection [73], and Page kidney [75]] and two were non-vascular [oral palsies [63] and atlantoaxial dislocation [74]]. Page kidney is a rare condition where compression from an external source triggers secondary hypertension. [76] No case reports described AEs as attributed to soft tissue techniques, exercise, or other physical modalities.
Risk of bias in studies
Table 3–9 One RCT was rated as high quality (low risk of bias), and the other five were rated as acceptable quality (moderate risk of bias) (Table 3). Three of the observational studies were scored as high quality (low risk of bias) and one was rated as acceptable quality (moderate risk of bias) (Table 4). All 15 case reports were described as high-quality by the JBI Critical Appraisal Checklist (Table 5). No studies were excluded for having a high risk of bias.
Results of individual studies
Data from the extracted RCTs are available in Table 6, observational studies in Table 7, and case reports in Table 8.
Reporting biasesAdverse event definitions
Four studies defined AEs as any new or worsening undesirable, untoward, or unfavorable effect [51, 52, 54, 55], two studies defined AEs as any undesirable medical event with new or significant exacerbation [35, 60], and three studies did not provide a definition [53, 61, 62] (Table 9). Pohlman et al. indicated the AE needed to be temporally associated intervention [55], and Dougherty et al. included events up to 30 days following study participation. [35] Gliedt et al. investigated specific serious adverse events, including vertebral artery dissection, cauda equina syndrome, fracture at site of SMT, and hardware failure at site of SMT. [57] Five studies included an adverse event grading scale. Goertz et al., Maiers et al., and Pohlman et al. the events as mild, moderate, severe, or serious [54, 55, 60], Dougherty et al. graded as mild, moderate, or severe [35], and Amorin-Woods et al. used a 1–5 grading scale consistent with mild, moderate, severe, life-threatening, and death. [51] Serious events were defined by these studies as occurrences resulting in death, hospitalization, significant disability, or incapacitation. [60, 61] The classification of AEs as ‘serious’ in these studies was consistent with our use of the ‘catastrophic’ grading category. [30]
Adverse event collection methods
Five studies used active surveillance with AEs collected at each session. [35, 54, 55, 60, 61] Active surveillance is an intentional and continuous process where safety information is sought from patients and providers through a prespecified collection process, as opposed to passive surveillance where AEs are more commonly reported voluntarily by providers. [77] In addition, Pohlman et al. used three content-validated questionnaires to assess AEs, with two completed by the patient and one by the provider. [55] Three studies used standardized self-reports forms but did not provide additional information on frequency or initiation process. [53, 61, 62] One study reported AEs through a customer service department complaint log, patient surveys and phone calls, and clinician reports [52], and another reported AEs from an incident register that tracks complaints and clinical incidents. [51] Gliedt et al. performed a retrospective chart review with cases identified through presence of surgical CPT codes and chiropractic CPT codes, with eligible charts searched for serious adverse events (i.e. vertebral artery dissection, cauda equina syndrome, fracture in location of SMT, and spine surgery hardware failure in location of SMT) occurring within 10 days following presenting for a chiropractic treatment. [57]
Discussion
We updated the 2017 systematic review [34] on adverse events following SMT and related chiropractic treatments of older adults and identified 19 new studies and case reports. Similar to the prior review, none of the RCTs or observational studies included in this update reported a catastrophic AE. All of the included studies described mild events (e.g., soreness), and there was limited reporting of moderate or severe events (e.g., rib fracture). The lack of catastrophic AEs following SMT is consistent with studies across ages [57, 78–80], suggesting that chiropractic AEs of mild severity are common, but life-threatening AEs are rare.
Our update included five new RCTs, two new observational studies, and 12 new case reports/series. Four studies from the 2017 review were excluded after not meeting the updated study design inclusion criteria [narrative review (n = 1), pilot study (n = 1), descriptive claims data (n = 2)]. None of those studies reported severe or catastrophic AEs, and their inclusion likely would not have substantially changed the findings in this report. Only two studies from the prior review met the updated inclusion criteria, accounting for just 41 of the 412 reported AEs we identified in this update, suggesting substantial growth in reporting of patient safety data for older adult patients since 2017.
By randomizing to minimize bias, use of strict protocols for monitoring, and using comparable groups to establish causation, RCTs are critical for identifying harms in clinical practice. [81] However, RCTs are limited in their ability to detect rare adverse events. [82] The included RCTs and observational cohort studies are powered to assess efficacy but were not adequately powered to observe rare AEs (e.g., cervical artery dissection). Case-control and population-based studies are more appropriate to detect rare events. [83] A 2015 analysis of U.S. Medicare Part B administrative data by Whedon et al. reported that the risk of traumatic injury within 7 days following a chiropractic office visit was increased for individuals with a chronic coagulation defect, inflammatory spondylopathy, osteoporosis, aortic aneurysm, and dissection, or long-term use of anticoagulant therapy. [21]
However, the risk of traumatic injury was low, and patients were 76% less likely to have an AE following a chiropractic office visit as compared to a primary care encounter. [21] A second 2015 Medicare B study of adults aged 66–99 years by Whedon et al. reported that the incidence of vertebrobasilar stroke following a chiropractic office visit was extremely low and comparable to those who saw a primary care physician. [38]
A study of Medicare Advantage health plan members’ administrative data by Koslof et al. corroborated Whedon et al., reporting no significant association between exposure to chiropractic care and vertebrobasilar artery stroke and concluded that SMT was unlikely to be a cause.
A 2025 Medicare claims data of 291,604 patients by Whedon et al. found that Medicare Part B beneficiaries with new onset neck pain were associated with lower rates of adverse events if the patient was seen by a chiropractor as compared to primary medical care. [85] Trager et al. utilized propensity-matching to investigate EHR data for fall risk of older adults (>65 years) following chiropractic visits and found that the SMT cohort had a lower fall risk than the non-SMT cohort but no difference in limb fracture risk. [86] Their analysis speculated that SMT may reduce fall risk through reducing pain and improving sensorimotor function, but advised caution in interpretation due to the observational design. [86] Like our included clinical studies, administrative and EHR population-based studies suggest that the incidence of severe or catastrophic events following chiropractic visits is rare.
Case reports are not appropriate to make statements about association or causation. [87] However, they were included because can serve as an “early warning system” and bring awareness to rare or previously unknown events that are potentially associated with treatment. [81] One of the case reports described an ICD shock following the application of a TENS unit over the thoracic region. The application of electrical stimulation devices over implantable devices (e.g., ICD, pacemaker) is contraindicated, and providers should be very cautious of applying in nearby regions. The other case reports described AEs following SMT, with them most commonly occurring in the cervical and lumbar regions. Low-impact manipulative treatments are generally thought of as safe, however, one AE described in a case report was following drop table manipulation [65] and two were following treatment with an Activator device. [64, 66] Ten of the cases were reported by chiropractors and ten by medical providers. The premise of one of the Activator case reports [64] was challenged and responded to in letters to the editor. [88–90]
Our results present a lack of standardization in the collection and reporting of AEs. There is a need for agreed-upon definitions to be utilized in both routine clinical practice and future investigations of manual therapy treatment harms. [27] An absence of standardized definitions and collection processes sets the stage for underreporting or misinterpretation of risk. The quality (risk of bias) of the included RCTs and observational studies did not appear to correspond to the number of AEs reported. Rather, the volume of AEs reported was dependent on the operational definition of AEs and the data collection methods (active versus passive) utilized. For example, Goertz et al. used active surveillance and identified 98 study related AEs in a study of 131 older adult patients [60], whereas, Amorin-Woods et al. used passive surveillance and identified only 20 AEs (6 in older adults) despite a population of 61,882 patients (all ages). [51]
In ambulatory care settings, the use of active surveillance AE reporting is feasible and results in the collection of significantly more AEs than passive surveillance. [91, 92] A call to action from the World Federation of Chiropractic Global Patient Safety Task Force urged the chiropractic profession to “develop transparent patient safety reporting information systems” with “standard vocabularies and common data models” to build a framework around patient safety. [42] Although it was beyond the scope of this study, the burden of increasing rates of disability secondary to back pain warrant studies to assess how chiropractors can best navigate adverse events in the clinic, educational opportunities to reduce events, and standardize reporting. [93]
Since 2017, there has been considerable growth in chiropractic patient safety literature for older adults (34). Only two studies from the prior review, an RCT (35) and a case series (37) met our inclusion criteria. In the present study, we identified an additional 23 articles over a 8–year period, representing an expansion in the literature on chiropractic treatments for older adults and the study of adverse events. Most of the included RCTs focused on lower back pain or related conditions, and more study is needed on chiropractic treatment approaches for older adults with other conditions (e.g., neck pain, thoracic pain, headaches, extremity conditions). Our study question focused solely on AEs following spinal manipulation treatment encounters with chiropractors. While we did not identify any reports of adverse events following soft tissue techniques or exercise, these approaches are frequently utilized by chiropractors in the management of older adults (6), and AEs for these approaches may be underreported or, in the case of multimodal care, misattributed to spinal manipulation. Future studies should be considered to investigate encounters with other manual therapy providers (e.g., physical therapists, massage therapists, osteopaths). Our study findings bolster the established safety profile for chiropractic treatments and may be utilized to reassure and guide policy makers, payors, and stakeholders in coverage determinations.
Limitations
There are several limitations to this systematic review. First, and most significantly, our search strategy focused on manipulation-related terminology, which means that most of the articles which were returned in our search focused on SMT. We opted not to search for specific terms for complementary therapies, physical therapy modalities, or rehabilitation interventions that are offered by both chiropractors and other manual therapy providers, such as dry needling, exercise therapy, TENS, or soft tissue therapy. This decision, while focusing our project on a manageable number of citations for screening, also meant that we may have missed important studies or case reports, although the use of the chiropract* wildcard likely captured articles otherwise not included. We encourage researchers planning future systematic reviews of chiropractic interventions to consider broadening their search terms to include these other treatments offered by chiropractors, and to plan their teams, methods, technology, timelines, and budgets to address the higher number of articles that will be returned. We also encourage researchers and clinicians to consider using more robust data collection systems to capture adverse events in their studies and practices for non-SMT treatments.
Secondly, we made two deviations from the protocol. Specifically, we included a study labeled as a pilot despite pilot studies being listed as an exclusion in the eligibility criteria. The study by Goertz et al. was initially excluded at the title/abstract screening phase but was then reconsidered following the urging of a study investigator (SS)(60). An a priori decision was made to exclude pilot studies because they are generally focused on trial feasibility and underpowered. Despite the Goertz article being titled as a pilot study, it was a large trial that was adequately powered, relevant to our research question, had incorporated an active surveillance process and AE grading classification system, and met all other eligibility criteria. Thus, a team decision was made to include it. It is possible that other pilot studies were excluded at the title/abstract screening phase that may have been relevant to our study. Second, we deviated from our protocol by adding two additional data items: AE operational definitions and approach to collecting AEs. The author team felt including this information provided needed context to frame the AE results of the clinical trials.
Next, we contacted the authors of eleven studies requesting individual patient data. For four of those studies, the authors either could not or would not share their data. It is unclear if their data included any adverse events in patients 55 years and older, or if the inclusion of the data would have impacted our study findings.
Another limitation is that we did not include non-clinical data such as administrative claims data, EHR data, or other databases (e.g., TriNetX). We did not include these sources because they are aggregate data sources that cannot provide granular patient data regarding case-level AEs. However, these study approaches are valuable in recognizing rare AEs, and we provided discussion as relevant to the safety of older adults.
When assessing study risk of bias, we numerically scored each item checklists item and used a percentage to determine overall quality. Scoring without weighting the items has the potential to oversimplify, mask critical flaws and provide misleading summaries of the study(94). Next, there is no consensus of definitions or terminology for classifying the severity of AEs. We decided a priori to use the terms mild, moderate, severe, and catastrophic based on recent conference proceedings and now published article reporting the results of an e-Delphi study(30,95). However, many of the included studies opted for the term serious over catastrophic, and we treated these terms interchangeably. We assigned severity of AE based on the rating provided in the studies and it is possible the severity was underreported by participating providers. Relatedness of the AE to the intervention also was based on the authors’ judgment, which might differ from the opinions of other adjudicators. That is, some AEs that were related to a chiropractic intervention might not have been labeled as such in the original paper and, therefore, would not have been included in our review. Lastly, we used the SIGN Cohort Checklist to assess the risk of bias in our observational studies. This checklist was designed with a focus on comparing cohorts and is not well suited to retrospective chart reviews(52) or single-arm cohort studies(55). Therefore, several items from the SIGN cohort checklist were not applicable to the cohorts that met inclusion criteria, and this may have impacted their risk of bias ratings.
Conclusion
Adverse events following chiropractic treatment services for older adults are common, with examples including changes in pain quality, muscle or joint soreness or stiffness, numbness, weakness, fatigue, headache, dizziness, or lightheadedness. No RCTs or cohort studies involving chiropractic treatment reported study-related catastrophic adverse events in older adults, and all studies reported mild or moderate AEs. The certainty of our findings is limited due to wide variability in the definition and collection process for AEs. Active surveillance of AEs in trials may lead to the identification of more AEs than are currently reported
Supplementary Material
Supplementary Material 1
Literature Search for Safety and adverse events associated
with chiropractic treatment services among older adults
Supplementary Material 2
Appendix A
Supplementary Material 3
Excluded papers and reasons
Supplementary Material 4
MANUSCRIPT REVISION CHECKLISTAcknowledgements
We would like to thank health sciences librarian Jennifer Smith for completing the PRESS checklist of our search strategy and providing feedback for revision. We would like to thank Lyndon Amorin-Woods, Eric Chun-Pu Chu, Roger Engel, Jordan Gliedt, Brent Leininger, Michele Maiers, Katie Pohlman, Craig Schulz, and Robert Trager, for generously sharing their adverse event patient data and answering clarification questions from our team.
Funding
Clinical Compass and NCMIC Foundation partially funded this study.
Authors and Affiliations
VA Puget Sound Health Care System, 9600 Veterans Drive SW, Tacoma, WA, USA
Clinton J. Daniels
University of Washington, Seattle, WA, USA
Clinton J. Daniels
American Chiropractic Association, Highland Park, IL, USA
Ronald J. Farabaugh
Palmer College of Chiropractic, Davenport, IA, USA
Stacie A. Salsbury & Maranda J Kleppe
Spectra Health, Grand Forks, ND, USA
Kristian R. Anderson
Private Practice, Santee, CA, USA
Wayne M. Whalen
Logan University, Chesterfield, MO, USA
Sheryl A. Walters
Private Practice, Bettendorf, IA, USA
Lisa Z. Killinger
VA Palo Alto Health Care System, San Jose, CA, USA
Alec L. Schielke
Contributions
ALS and CJD conceptualized the study and drafted the protocol.
ALS registered the protocol.
ALS, CJD, and SAW designed the search strategy.
RJF, LZK, and CJD screened the articles.
KRA, RJF, MK, SAS, and CJD extracted the articles and performed risk of bias assessments.
CJD drafted the manuscript.
All authors reviewed the manuscript, provided critical feedback, and approved the submission.
Competing interests
The authors acknowledge the following competing interests.
CJD, RJF, SAS, WMW, SAW, and ALS are all members of the Clinical Compass Scientific Commission.
The efforts of CJD and ALS were partially funded through Clinical Compass. The Clinical Compass Executive Board approved initiation of the study but did not have any input or oversight of the study design or or conduct.
SAS serves in a voluntary capacity for the World Federation of Chiropractic Research Committee and is a member of the WFC Global Patient Safety Initiative Executive Committee.
SAS is a member of the editorial board of Chiropractic & Manual Therapies and serves as a guest editor for a special collection on patient safety; she had no involvement in the editorial decisions related to this manuscript.
SAS reports research grant funding outside the submitted work from the U.S. National Institutes of Health—National Center for Complementary and Integrative Health (paid to Palmer College of Chiropractic) and travel support for research presentations from Parker Seminars.
SAS and MK report funding unrelated to this project from RAND Research Pilot Grants. Palmer Center for Chiropractic Research provided in-kind support for SAS and MK.
The authors have no additional relevant financial conflicts of interest to disclose.
References:
Funabashi M, Holmes MM, Pohlman KA, Salsbury S, O’Beirne M, et al.
"Doing Our Best for Patient Safety": An International and
Interprofessional Qualitative Study with Spinal Manipulative
Therapy Providers in Community-based Settings
Musculoskelet Sci Pract 2021 (Dec): 56: 102470Practice Analysis of Chiropractic - 2025
National Board of Chiropractic ExaminersWright DS, Kleppe M, Coleman BC, Funabashi M, et al.
Patient Safety Culture Research Within the
Chiropractic Profession: A Scoping Review
Chiropractic & Manual Therapies 2025 (Oct 21); 33: 46Minetto MA, Giannini A, McConnell R, Busso C, Torre G.
Common musculoskeletal disorders in the elderly:
the star triad.
J Clin Med. 2020;9(4):1216.Beliveau PJH, Wong JJ, Sutton DA, et al.
The Chiropractic Profession: A Scoping Review of
Utilization Rates, Reasons for Seeking Care,
Patient Profiles, and Care Provided
Chiropractic & Manual Therapies 2017 (Nov 22); 25: 35de Luca K, Hogg-Johnson S, Funabashi M, Mior S, French SD.
The Profile of Older Adults Seeking Chiropractic Care:
A Secondary Analysis
BMC Geriatrics 2021 (Apr 23); 21 (1): 271Wong CK, Mak RY, Kwok TS, et al.
Prevalence, incidence, and factors associated with non-specific
chronic low back pain in community-dwelling older adults
aged 60 years and older: a systematic review
and meta-analysis.
J Pain. 2022;23(4):509–24.GBD 2021 Neck Pain Collaborators.
Global, regional, and national burden of neck pain, 1990-2020,
and projections to 2050: a systematic analysis of the
Global Burden of Disease Study 2021.
Lancet Rheumatol. 2024;6(3):e142–55.GBD 2021 Osteoarthritis Collaborators.
Global, Regional, and National Burden of Osteoarthritis,
1990-2020 and Projections to 2050: A Systematic Analysis
for the Global Burden of Disese Study 2021
Lancet Rheumatol 2023 (Aug 21); 5 (9): e508–e522Ferreira ML, de Luca K.
Spinal pain and its impact on older people.
Best Pract Res Clin Rheumatol. 2017;31(2):192–202.Mills SEE, Nicolson KP, Smith BH.
Chronic pain: a review of its epidemiology and
associated factors in population-based studies.
Br J Anaesth. 2019;123(2):e273–83.e Luca KE, Parkinson L, Haldeman S, Byles JE, Blyth F.
The Relationship Between Spinal Pain and Comorbidity:
A Cross-sectional Analysis of 579 Community-Dwelling,
Older Australian Women
J Manipulative Physiol Ther 2017 (Sep); 40 (7): 459–466Yang H, Haldeman S, Hurwitz EL, Tavares PA, et al.
Association of cognitive impairment and spinal pain in the
older adult population in the United States:
a cross-sectional study.
J Manipulative Physiol Ther. 2025.
https://doi.org/10.1016/j.jmpt.2025.07.001.Chu ECP, Trager RJ.
Prevalence of serious pathology among adults with low back
pain presenting for chiropractic care: a retrospective
chart review of integrated clinics in Hong Kong.
Med Sci Monit. 2022;28:e938042-1-e938042-10 (Sept 27).Puac-Polanco P, Rodriguez A, Hiremath S, Riascos RF, Torres C.
Traumatic and Nontraumatic Spine Emergencies in Geriatric
Patients. In: Atlas of Emergency Imaging from Head-to-Toe
[Internet]. Springer, Cham; 2025 [cited 2025 Sept 17]. p. 877–92.
Available from: https://link.springer.com/rwe/
https://doi.org/10.1007/978-3-031-78916-8_54Leung DKY, Fong APC, Wong FHC, et al.
Nonpharmacological interventions for chronic pain in
older adults: a systematic review and meta-analysis.
Gerontologist. 2024;64(6):gnae010.Chou R, Deyo R, Friedly J, Skelly A, Hashimoto R, et al.
Nonpharmacologic Therapies for Low Back Pain:
A Systematic Review for an American College
of Physicians Clinical Practice Guideline
Annals of Internal Medicine 2017 (Apr 4); 166 (7): 493–505Qaseem A, Wilt TJ, McLean RM, Forciea MA.
Noninvasive Treatments for Acute, Subacute, and Chronic
Low Back Pain: A Clinical Practice Guideline
From the American College of Physicians
Annals of Internal Medicine 2017 (Apr 4); 166 (7): 514–530Whedon JM, Kizhakkeveettil A, Toler AW, Bezdjian S, et al.
Initial Choice of Spinal Manipulation Reduces
Escalation of Care for Chronic Low Back Pain
Among Older Medicare Beneficiaries
Spine (Phila Pa 1976) 2022 (Feb 15); 47 (4): E142–E148Bagagiolo D, Persiani M, Cicchitti L, Vismara L, et al.
Efficacy and safety of musculoskeletal manipulations in
elderly population with musculoskeletal disorders:
a systematic review.
BMJ Open. 2025;15(6):e088655.Whedon JM, Mackenzie TA, Phillips RB, Lurie JD.
Risk of Traumatic Injury Associated with Chiropractic
Spinal Manipulation in Medicare Part B
Beneficiaries Aged 66-99
Spine (Phila Pa 1976) 2015 (Feb 15); 40 (4): 264–270Gielen E, Dupont J, Dejaeger M, Laurent MR.
Sarcopenia, osteoporosis and frailty.
Metabolism. 2023;145:155638.Grabowska W, Burton W, Kowalski MH, et al.
A Systematic Review of Chiropractic Care for Fall Prevention: Rationale,
State of the Evidence, and Recommendations
for Future Research
BMC Musculoskelet Disord 2022 (Sep 5); 23 (1): 844World Health Organization.
WHO Guidelines on Basic Training and Safety in Chiropractic
Geneva 2005Whalen W, Hawk C, Farabaugh R, Daniels C, et al.
Best Practices for Chiropractic Management of
Adult Patients With Mechanical Low Back Pain:
A Clinical Practice Guideline for
Chiropractors in the United States
J Manipulative Physiol Ther 2022 (Oct); 45 (8): 551-565Whalen W, Farabaugh R, Hawk C, et al.
Best-Practice Recommendations for Chiropractic
Management of Patients With Neck Pain
J Manipulative Physiol Ther. 2019 (Nov); 42 (9): 635–650Funabashi M, Gorrell LM, Pohlman KA, Bergna A, Heneghan NR.
Definition and Classification for Adverse Events
Following Spinal and Peripheral Joint
Manipulation and Mobilization:
A Scoping Review
PLoS One 2022 (Jul 15); 17 (7): e0270671Funabashi M, Pohlman KA, Gorrell LM, Salsbury SA, Bergna A.
Expert Consensus on a Standardised Definition and Severity
Classification for Adverse Events Associated with Spinal
and Peripheral Joint Manipulation and Mobilisation:
Protocol for an International E-Delphi Study
BMJ Open 2021 (Nov 11); 11 (11): e050219Carlesso LC, Cairney J, Dolovich L, Hoogenes J.
Defining adverse events in manual therapy:
an exploratory qualitative analysis
of the patient perspective.
Man Ther. 2011;16(5):440–6.Funabashi M, Gorrell LM, Pohlman KA, Bergna A.
Defining and Classifying Adverse Events Following Joint
Manipulation and Mobilization: An International
e-Delphi Study and Focus Groups
PLoS One 2025 (Nov 17); 20 (11): e0334151Swait G, Finch R.
What Are the Risks of Manual Treatment of the Spine?
A Scoping Review for Clinicians
Chiropractic & Manual Therapies 2017 (Dec 7); 25: 37To D, Tibbles A, Funabashi M.
Lessons learned from cases of rib fractures after
manual therapy: a case series to increase patient safety.
J Can Chiropr Assoc. 2020;64(1):7–15.Hawk C, Schneider M, Dougherty P, Gleberzon BJ, Killinger LZ.
Best Practices Recommendations for Chiropractic Care
for Older Adults: Results of a Consensus Process
J Manipulative Physiol Ther 2010 (Jul); 33 (6): 464–473Hawk C, Schneider MJ, Haas M, Katz P, Dougherty P, Gleberzon B, et al.
Best Practices for Chiropractic Care for Older Adults:
A Systematic Review and Consensus Update
J Manipulative Physiol Ther 2017 (May); 40 (4): 217–229Dougherty PE, Karuza J, Dunn AS, Savino D, Katz P.
Spinal Manipulative Therapy for Chronic Lower Back Pain
in Older Veterans: A Prospective, Randomized,
Placebo-Controlled Trial
Geriatric Orthopaedic Surgery and Rehab. 2014 (Dec); 5 (4): 154–164Cambron JA, Schneider M, Dexheimer JM, Iannelli G, et al.
A pilot randomized controlled trial of flexion-distraction
dosage for chiropractic treatment of lumbar spinal stenosis.
J Manipulative Physiol Ther. 2014;37(6):396–406.Dougherty PE, Engel RM, Vemulpad S, Burke J.
Spinal manipulative therapy for elderly patients with
chronic obstructive pulmonary disease: a case series.
J Manipulative Physiol Ther. 2011;34(6):413–7.Whedon JM, Song Y, Mackenzie TA, et al.
Risk of Stroke After Chiropractic Spinal Manipulation
in Medicare B Beneficiaries Aged 66 to 99 Years
With Neck Pain
J Manipulative Physiol Ther. 2015 (Feb); 38 (2): 93–101Gleberzon BJ.
A narrative review of the published chiropractic
literature regarding older patients from 2001-2010.
J Can Chiropr Assoc. 2011;55(2):76–95.Moore C, de Luca K, Wong AYL, Fernandez M, Swain M, Hartvigsen J, et al.
Characteristics of chiropractors who manage people aged 65
and older: a nationally representative sample
of 1903 chiropractors.
Australas J Ageing. 2019;38(4):249–57.Trager RJ, Bejarano G, Perfecto RPT, Blackwood ER, Goertz CM.
Chiropractic and Spinal Manipulation: A Review
of Research Trends, Evidence Gaps,
and Guideline Recommendations
J Clin Med 2024 (Sep 24); 13 (19): 5668Coleman BC, Rubinstein SM, Salsbury SA, Swain M, Brown R, Pohlman KA.
The world federation of chiropractic global patient
safety task force: a call to action.
Chiropr Man Therap. 2024;32(1):15.Schielke A, Walters S, Daniels C, et al.
PROSPERO: international prospective register of
systematic reviews. [cited 2025 June 14].
afety and adverse events associated with chiropractic
reatment services among older adults.
Available from: https://www.crd.york.ac.uk/
PROSPERO/view/CRD42024629286Page MJ, McKenzie JE, Bossuyt PM, Boutron I, et al.
The PRISMA 2020 statement: an updated guideline
for reporting systematic reviews.
BMJ. 2021;372:n71.Learman KE, Showalter C, O’Halloran B, Cook CE.
Thrust and nonthrust manipulation for older adults with
low back pain: an evaluation of pain and disability.
J Manipulative Physiol Ther. 2013;36(5):284–91.Zulman DM, Sussman JB, Chen X, Cigolle CT.
Examining the evidence: a systematic review of the inclusion
and analysis of older adults in randomized controlled trials.
J Gen Intern Med. 2011;26(7):783–90.De la Ruelle LP, de Zoete A, Myburgh C, Brandt HE, Rubinstein SM.
The Perceived Barriers and Facilitators for Chiropractic
Care in Older Adults with Low Back Pain; Insights
from a Qualitative Exploration in a Dutch Context
PLoS One 2023 (Apr 12); 18 (4): e0283661Vigdal ŘN, Storheim K, Munk Killingmo R, Smĺstuen MC, Grotle M.
Characteristics of Older Adults with Back Pain Associated with
Choice of First Primary Care Provider: A Cross-sectional
Analysis from the BACE-N Cohort Study
BMJ Open 2021 (Sep 17); 11 (9): e053229Jenkins HJ, Grace K, Young A, Parker F, Hartvigsen J, et al.
Diagnostic imaging in the management of older adults with
low back pain: analysis from the BAck Complaints in Elders:
Chiropractic - Australia cohort study.
Chiropr Man Therap. 2024;32(1):40.Ouzzani M, Hammady H, Fedorowicz Z, Elmagarmid A.
Rayyan – a web and mobile app for systematic reviews.
Syst Rev. 2016;5:210.Amorin-Woods LG, Cascioli V, Losco BE, Parkin-Smith GF.
Adverse events reported across 15 years of multicenter
chiropractic student clinical placements
in Western Australia.
J Patient Saf. 2025;21(5):329–38.Chu EC, Trager RJ, Lee LY, Niazi IK.
A Retrospective Analysis of the Incidence of
Severe Adverse Events Among Recipients of
Chiropractic Spinal Manipulative Therapy
Sci Rep 2023 (Jan 23); 13 (1): 1254Bronfort G, Maiers M, Schulz C, Leininger B, et al.
Multidisciplinary Integrative Care Versus Chiropractic Care
for Low Back Pain: A Randomized Clinical Trial
Chiropractic & Manual Therapies 2022 (Mar 1); 30: 10Maiers M, Hartvigsen J, Evans R, Westrom K, et al.
Short or long-term treatment of spinal disability in
older adults with manipulation and exercise.
Arthritis Care Res (Hoboken). 2019;71(11):1516–24.Pohlman KA, Funabashi M, O’Beirne M, Cassidy JD, et al.
What's the Harm? Results of an Active Surveillance
Adverse Event Reporting System for
Chiropractors and Physiotherapists
PLoS One 2024 (Aug 19); 19 (8): e0309069Engel RM, Bailey R, Luker C, Parry A, Graham P, Grace S.
The effect of manual therapy and low intensity exercise
on lung function and quality of life in healthy adults
between 50 and 65 years: a randomised controlled trial.
J Aust Tradit-Med Soc. 2020;26(3):158–63.Gliedt JA, Gruttke J, Jones A, King J, Spector AL, et al.
A description of serious adverse events following spinal
manipulative therapy for adults with history of spine surgery:
a single institution retrospective chart review.
J Man Manip Ther. 2025;3:1–11.Scottish Intercollegiate Guideline Network (SIGN).
Methodology checklists [Internet]. 2021
[cited 2024 June 12]. Available from:
https://www.sign.ac.uk/using-our-
guidelines/methodology/checklists/Moola S, Munn Z, Tufanaru C, Aromataris E.
Chapter 7: Systematic reviews of etiology and risk.
In: Joanna Briggs Institute Reviewer’s Manual [Internet].
The Joanna Briggs Institute; 2017. Available from:
https://reviewersmanual.joannabriggs.org/Goertz CM, Salsbury SA, Long CR, Vining RD, et al.
Patient-centered Professional Practice Models
for Managing Low Back Pain in Older Adults:
A Pilot Randomized Controlled Trial
BMC Geriatr. 2017 (Oct 13); 17 (1): 235Schneider MJ, Ammendolia C, Murphy DR, Glick RM, et al.
Comparative Clinical Effectiveness of Nonsurgical Treatment
Methods in Patients With Lumbar Spinal Stenosis:
A Randomized Clinical Trial
JAMA Netw Open 2019 (Jan 4); 2 (1): e186828Schulz C, Evans R, Maiers M, Schulz K, Leininger B, Bronfort G.
Spinal Manipulative Therapy and Exercise for Older Adults
with Chronic Low Back Pain: A Randomized Clinical Trial
Chiropractic & Manual Therapies 2019 (May 15); 27: 21 .Baruch O.
A rare combination of unilateral transient vocal cord,
soft palate, and tongue palsies and numbness following
chiropractic manipulation to the cervical spine:
a case report.
J Int Acad Neuromusculoskel Med. 2023;20(2):19–31.Cohen FL.
Cerebral hemorrhage following chiropractic Activator
treatment - case report and review of literature.
J Neurol Surg Rep. 2016;77(4):e162–7.Etebari C, Yanamala S, Dubin J.
A Case Report of U-Type Sacral Fracture
After Chiropractic Adjustment.
JBJS Case Connect. 2023;13(4).Garcia D, Nottmeier E, Pirris S.
Transient neuropathic pain following mechanically assisted
manipulation of the spine: a clinical case study.
Cureus. 2023;15(8):e42912.Hall DA, Fraint A, Dafer R.
Acute stroke in middle cerebellar peduncle in
a patient with FXTAS.
Front Genet. 2018;9:187.Ko KY, Kim SE, Hwang JW, Namgung J, Cho SW.
Delayed cardiac perforation caused by pacemaker
lead dislodgement during chiropractic therapy.
JACC Case Rep. 2025;30(20):104192.Liu H, Zhang T, Qu T, Yang CW, Li SK.
Spinal epidural hematoma after spinal manipulation
therapy: Report of three cases and a literature review.
World J Clin Cases. 2021;9(22):6501–9.Paulus YM, Belill N.
Preretinal hemorrhages following chiropractor
neck manipulation.
Am J Ophthalmol Case Rep. 2018;11:181–3.Shenoy A, Sharma A, Achamyeleh F.
Inappropriate ICD discharge related to electrical
muscle stimulation in chiropractic therapy:
a case report.
Cardiol Ther. 2017;6(1):139–43.Skappak C, Saude EJ.
Back pain in the emergency department: pathological
fracture following spinal manipulation.
CJEM. 2018;20(2):307–12.Szafran K, Zheng Y, Butensky F.
Vertebral artery dissection following high velocity
low amplitude cervical manipulation: a case report.
Cureus. 2025;17(7):e87689.Tsou A, Juan YH, Chen TY, Lin SK.
Thrombolysis for atlantoaxial dislocation
mimicking acute ischemic stroke.
Am J Emerg Med. 2019;37(6):1216.e3-1216.e5.Wahdat R, Schwartz C, Espinosa J, Lucerna A.
Page kidney: taking a page from history.
Am J Emerg Med. 2017;35(1):193.e1-193.e2.Lind CA, Tjiattas-Saleski L.
Exploration of hypertension following traumatic renal
hematoma formation and Page kidney discussion.
Cureus. 2024;16(5):e60468.Organization WH.
The importance of pharmacovigilance [Internet].
World Health Organization; 2002 [cited 2025 June 24].
Available from: https://iris.who.int/handle/10665/42493Weis CA, Stuber K, Murnaghan K, Wynd S.
Adverse events from spinal manipulations in the pregnant
and postpartum periods: a systematic review and update.
J Can Chiropr Assoc. 2021;65(1):32–49.Pankrath N, Nilsson S, Ballenberger N.
Adverse events after cervical spinal manipulation -
a systematic review and meta-analysis of
randomized clinical trials.
Pain Physician. 2024;27(4):185–201.Gorrell LM, Brown BT, Engel R, Lystad RP.
Reporting of Adverse Events Associated with Spinal
Manipulation in Randomised Clinical Trials:
An Updated Systematic Review
BMJ Open 2023 (May 4); 13 (5): e067526Riley DS, Barber MS, Kienle GS, Aronson JK, et al.
CARE guidelines for case reports: explanation
and elaboration document.
J Clin Epidemiol. 2017;89:218–35.Thynne TR, Gabb GM.
Limitations of randomised controlled trials
as evidence of drug safety.
Aust Prescr. 46(2):22–3.Dey T, Mukherjee A, Chakraborty S.
A practical overview of case-control
studies in clinical practice.
Chest. 2020;158(1S):S57-64.Kosloff TM, Elton D, Shulman SA, Clarke JL, Skoufalos A, Solis A.
Conservative Spine Care: Opportunities to
Improve the Quality and Value of Care
Popul Health Manag. 2013 (Dec); 16 (6): 390–396Whedon JM, Anderson B, Mackenzie TA, Grout L, et al.
Observational Study of the Safety of Chiropractic
vs Medical Care Among Older Adults With Neck Pain
J Manipulative Physiol Ther 2025 (Sep 9): S0161-4754(25)00002-8Trager RJ, Burton WM, et al.
Chiropractic spinal manipulation and fall risk in older
adults with spinal pain: observational findings
from a matched retrospective cohort study.
Cureus. 2024;16(10):e72330.Nissen T, Wynn R.
The clinical case report: a review of
its merits and limitations.
BMC Res Notes. 2014;7(1):264.Tuchin PJ.
Cerebral hemorrhage following chiropractic activator
treatment: case report and review of literature.
J Neurol Surg Rep. 2017;78(3):e113–4.Liebschner MAK, Ehni BL.
Letter to the editor: cerebral hemorrhage following
chiropractic activator treatment-case report
and review of literature.
J Neurol Surg Rep. 2017;78(4):e115–6.Cohen FL.
Author’s response to letter to the editor:
cerebral hemorrhage following chiropractic
activator treatment-case report and
review of the literature.
J Neurol Surg Rep. 2017;78(4):e117–8.Pohlman KA, Carroll L, Tsuyuki RT, Hartling L, Vohra S.
Comparison of active versus passive surveillance
adverse event reporting in a paediatric ambulatory
chiropractic care setting: a cluster
randomised controlled trial.
BMJ Open Qual. 2020;9(4):e000972.Pohlman KA, Funabashi M, Ndetan H, Hogg-Johnson S.
Assessing adverse events after chiropractic care
at a chiropractic teaching clinic:
an active-surveillance pilot study.
J Manipulative Physiol Ther. 2020;43(9):845–54.GBD 2021 Low Back Pain Collaborators.
Global, Regional, and National Burden of Low Back Pain,
1990–2020, Its Attributable Risk Factors, and
Projections to 2050: A Systematic Analysis of
the Global Burden of Disease Study 2021
Lancet Rheumatology 2023 (May 23); 5 (6): E316-E329Siedler MR, Kawtharany H, Azzam M, Ezgü D, et al.
Risk of bias assessment tools often addressed items not
related to risk of bias and used numerical scores.
J Clin Epidemiol. 2025;1(180):111684.Funabashi M, Gorrell L, Pohlman K, Bergna A, Heneghan N.
Adverse Events (AE) Following Joint Manipulation and
Mobilization: An International e-Delphi Study
and Focus Groups to Define and Classify these AEs.
In: 2024 International Congress on Integrative Medicine & Health Abstracts. 2024.
Return to ADVERSE EVENTS
Since 4-10-2026
| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |